

 PDF
PDF Citation
Citation Print
Print



Nowadays lumbar laminectomy is a common surgery in daily practice and a very safe procedure, but it can result in sudden life threatening though infrequent vascular complications with greater than 50% mortality [1]. Such events usually require immediate intervention, so it is essential that anesthesiologists and surgeons be aware of this potential complication, its manifestation and treatment. The incidence of iatrogenic vascular complications in lumbar spine surgery is reported to be 0.01%-0.17% [1]. Although reported cases are few, unrecognised events are more than expected. However when one such event does occur, it can cause fatality in an otherwise healthy patient.
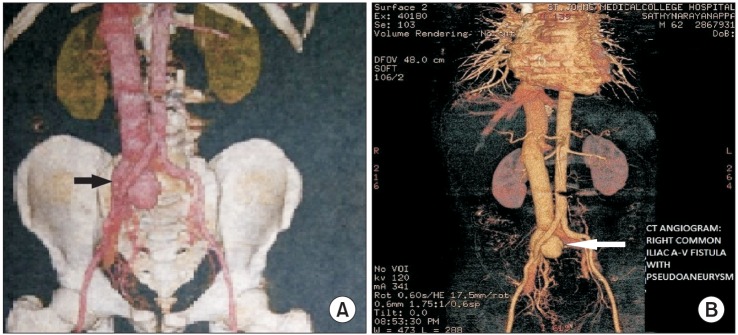
We present a case of a 55-years-old male, American Society of Anesthesiologists physical status I with low backache since 10 years, underwent laminectomy and screw fixation for the same. On the ninth postoperative day he started developing right lower limb swelling associated with pain. Deep vein thrombosis was ruled out on venous doppler. On postoperative day 15, he started developing dyspnea, and generalized edema. Abdominal bruit was present and neck veins were engorged. On postoperative day 16, facial edema increased and hypotension developed. CT angiogram of chest and abdomen revealed distal right common iliac artery fistulous communication with common iliac vein with prominent inferior vena cava and hepatic vein, pseudo-aneurysm arising from site of fistula (4.2 × 3.8 × 3.1 cc), neck of aneurysm measuring 18.5 mm (Fig. 1). CT chest showed bilateral pleural effusion with ground glass opacities. Emergency aneurysm repair was done on the same day. Postoperatively he was shifted to the surgical intensive care unit for elective ventilation and monitoring due to massive fluid shifts intra-operatively and massive hemorrhage. He was later hemodynamically stable and kept in intensive care unit for 3 more days and subsequently shifted to ward on postoperative day 4. Further course in ward was uneventful and the patient was discharged on postoperative day 7.
The L4-5 disc space is the most common site for a herniation of intervertebral disc [2]. Bifurcation of the aorta and inferior vena cava lies just anterior to this disc space, separated from it only by the anterior spinal ligament. The pathogenesis of iatrogenic vascular injury after spinal injury relates to the anatomical complexity of the aortic bifurcation and inferior vena cava confluence occurring at or below L4. They may present immediately in the intraoperative period or remain subclinical for days to years [3]. Bleeding from the wound is not a reliable sign as the self-sealing effect of the anterior annulus fibrosus and anterior longitudinal ligament may prevent any bleeding to be seen posteriorly. These tissues are tough and elastic, leading to blood leakage in the retroperitoneal space rather than the operating field. Signs and symptoms are equally wide ranging and include intra-operative and postoperative hypotension, associated fall in hematocrit, acute ischemia, distal pulse deficit, bruit, thrill, pulsatile abdominal mass, abdominal pain, expanding hematoma, limb edema and non-healing wounds. As the arterial injury drain directly into the low pressure venous system, hemorrhage is an uncommon presentation with arteriovenous fistula and hence it becomes very difficult to identify such injuries. An arteriovenous fistula should be suspected in a patient with a history of lower lumbar disc surgery followed by progressive swelling of a lower limb and associated bruit [4]. Thus, a high index of suspicion is needed amongst anesthesiologists given the rarity of complications and wide range of presentations.
 XML Download
XML Download