

 PDF
PDF Citation
Citation Print
Print


Introduction
Fentanyl is routinely used before induction of anesthesia, for intraoperative analgesia, and as a premedication to ameliorate the sympathetic response to laryngoscopy and intubation. Opioid agonists are known to possess antitussive activity, although intravenous (IV) administration of fentanyl, a synthetic opioid made soluble in a citrate-binding form, paradoxically induces cough. Fentanyl-induced cough (FIC) in most patients is usually benign, transient, and self-limiting; however, it may sometimes be spasmodic or explosive and life-threatening, requiring immediate intervention [12]. The reported incidence of FIC is quite variable (18%–65%) depending on the dose and route of administration of fentanyl [3456]. Increased intracranial, intraocular, and intra-abdominal pressures due to reflex coughing can be hazardous in patients undergoing surgery, especially for neurosurgical and ophthalmic procedures.
Nonpharmacological treatments to prevent FIC may help to reduce the cost of treatment and decrease hospital stays. Dilution of fentanyl has been proven to help prevent FIC [7] and is a standard practice at our institute. Acupressure also appears to prevent FIC because it has a proven role in the treatment of cough [89] and is easy to apply to specific points.
The primary aim of this study was to investigate whether acupressure applied to specific points before giving fentanyl is superior to dilution of fentanyl in reducing the incidence of FIC. The secondary aim was to determine the incidence of FIC in female patients at our cancer care institute.
Materials and Methods
This prospective randomized controlled study was conducted following approval from the institutional ethical committee (P. N. 1241, Dated: February 10, 2014). This study was registered in the clinical trial registry of India (CTRI/2014/03/004467) prior to the patients' enrollment. Written informed consent was obtained from all patients the day before the surgical procedure. The study included 225 female patients aged 18 to 60 years with American Society of Anesthesiologists physical status of I or II who were undergoing an elective oncological surgery (breast cancer surgeries, bone and soft tissue cancer surgeries, gyno-oncological and uro-oncological surgeries) under general anesthesia. Patients with a history of smoking, asthma, chronic obstructive pulmonary disease, upper respiratory tract infection in the previous 2 weeks, previous bronchodilator or steroid therapy, treatment with angiotensin-converting enzyme inhibitors, a history of drug/opioid abuse, and a known hypersensitivity to fentanyl were excluded. Patients with lung or head and neck malignancies who were anticipated to have difficult airway intubation were also excluded.
The sample size was based on a 35% reported incidence of cough after an IV bolus of undiluted fentanyl, assuming that acupressure and dilution will individually reduce the incidence of coughing from 35% to 15%. With an α value of 0.05 and β value of 0.20, the sample size was 71 patients in each group; we decided to include 75 patients in each group to account for any dropouts. The patients were randomly divided into 3 groups of 75 each using a computer-generated table of random numbers.
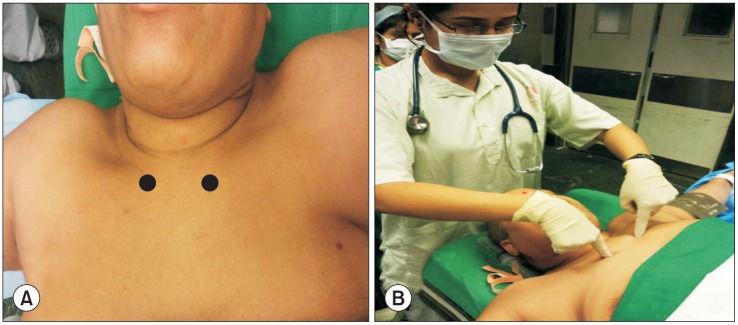
In the operating room, standard electrocardiography, noninvasive blood pressure, and pulse oximetry were monitored and baseline parameters were noted. Venous access was secured using a 20- or 22-G cannula on the dorsal hand. In the control group, patients received undiluted fentanyl at 3 µg/kg IV over a period of 3 seconds from the nearest port of the IV cannula. Patients in the acupressure group received undiluted fentanyl at 3 µg/kg IV over a period of 3 seconds from the nearest port of the IV cannula, with acupressure. All patients were informed about the nature of the applied pressure. Acupressure was applied 30 seconds before administration of fentanyl at the K 27 points (Fig. 1A), below the medial ends of the clavicles on either side of the manubrium sterni (Elegant Manson) [89] using two index fingers (Fig. 1B). Acupressure was continuous for 1 minute following administration of fentanyl. The pressure applied was tolerable for the patients. In the dilution group, patients received diluted fentanyl at 3 µg/kg IV over a period of 3 seconds from the nearest port of the IV cannula without acupressure. Fentanyl was diluted to 10 µg/ml with 0.9% normal saline. No other drugs were given before administration of fentanyl. No preoxygenation or breathing exercises were performed in the operating room before giving fentanyl. The primary outcomes were the incidence and severity of FIC. Blinding of the researchers was achieved by placing a surgical drape over the chest and a screen at the head end of the table. Coughing was observed by another anesthesiologist who was blinded to the patients' group allocation. The anesthesiologist involved in induction and maintenance of anesthesia was also blinded to the group allocation. Any episode of cough within 2 min of fentanyl administration was classified as FIC. The severity of FIC was graded as follows: mild, 1 to 2 coughs; moderate, 3 to 4 coughs; and severe, ≥ 5 coughs. The timing of the cough from drug administration was noted in each patient.
Any change in mean arterial pressure, heart rate, electrocardiography, and chest rigidity was recorded. Vital parameters were noted every minute until 5 minutes before and after fentanyl administration and every 5 minutes for 30 minutes. After 5 minutes of observation, anesthesia was induced with IV propofol at 1.5 to 2.5 mg/kg. Muscle relaxants and tracheal intubation were used according to the requirements of the specific surgical procedure. Patients were monitored throughout the surgery using standard monitoring.
Statistical analysis
Demographic and clinical variables are presented as frequency (percentage) and mean (SD) or median as appropriate. Group comparisons (acupressure and dilution of fentanyl) were made using the independent t-test according to the distribution of the data for continuous variables. Comparisons among more than two groups (control group, acupressure group, and dilution group) were made using ANOVA according to the distribution of the data for continuous variables. Categorical variables (acupressure and dilution of fentanyl along with FIC grade, nausea, vomiting, etc.) were analyzed using the chi-square test or Fisher's exact test (for binary variables). Correlations between the different scales were compared with Pearson correlation and Crammers V correlation for categorical variables. A P value of < 0.05 was considered to indicate statistical significance.
Results
In total, 276 female patients were screened. Fifty-one patients were excluded from the study because of a history of asthma, tobacco chewing/smoking, upper respiratory tract infection, treatment with angiotensin-converting inhibitors, obesity, or failure to provide consent. Therefore, 225 patients were included in the study, and 75 patients were randomized to each group. However, five patients were excluded from the final analysis because of study protocol violations. The demographic profile of the patients was similar across all three groups (Table 1).
The incidence of FIC was 12.7% (9 of 71 patients coughed) in the control group, 6.8% (5 of 74 patients) in the dilution group, and 1.3% (1 of 75 patients) in the acupressure group. The difference in the incidence of cough was statistically significant (P = 0.008) between the control and acupressure groups. There was no significant difference between the control and dilution groups or between the acupressure and dilution groups. The difference in the severity of cough among the groups was not statistically significant. The median onset time of cough in all groups was 9 to 12 seconds, with all coughs occurring within 30 seconds (Table 2). There was no significant difference in the mean arterial pressure or heart rate at baseline, before injection, or at 1, 3, 5, 10, 15, or 30 minutes in the 220 patients or in the 15 patients who coughed (P > 0.05). There was no chest rigidity in any patient.
Discussion
Our study demonstrated a reduced incidence of FIC associated with acupressure applied prior to fentanyl administration (1.3%) and with dilution of fentanyl (6.8%) as compared to 12.7% in the control group. There are practically no data on the incidence of FIC in the female population or in cancer patients. The incidence of FIC in the present study was lower (12.7%) than that reported in the literature (18%–65%) [3456]. This may be due to the female sex or the lower incidence of FIC in cancer patients. Previous studies showed that capsaicin cough sensitivity is higher in female patients [1011]. Oshima et al. [12] found no difference in the probability of FIC based on sex.
The cough reflex comprises an afferent limb consisting of receptors and afferent nerves, the cough center in the brain stem, and an efferent pathway consisting of motor nerves supplying the muscles involved in coughing. FIC is an involuntary act triggered by fentanyl and is occasionally severely explosive and spasmodic. Pulmonary C-fiber receptors, also known as Jreceptors, are present in the lower respiratory tract, and along with the nonmyelinated afferent fibers are most likely involved in the mediation of the pulmonary chemoreflex that leads to FIC [51314]. J-receptors are readily accessible via the pulmonary circulation and are more sensitive to chemical irritants [1516]. Fentanyl constricts tracheal smooth muscle, thereby stimulating the "irritant" receptors in the mucosa and triggering cough due to deformation of the tracheobronchial wall [17].
Bohrer et al. [5] reported a 45.9% incidence of FIC. Patients were scheduled for coronary artery bypass grafting and received fentanyl at 7 µg/kg via a central venous catheter. The mean onset time from the end of fentanyl administration to the beginning of coughing was 10.6 seconds. The incidence of FIC in another study was 28% when 1.5 µg/kg of fentanyl was given via a peripheral venous cannula [6]. The researchers also noted that this response to fentanyl was not altered by premedication with atropine or midazolam but was reduced after morphine (P < 0.01), whereas the incidence of FIC was as high as 65% after a 2.5 µg/kg IV fentanyl bolus injection [4]. There are numerous methods of preventing FIC, including pharmacological and nonpharmacological methods such as IV lidocaine [41418]; the huffing maneuver [19]; aerosol drugs such as salbutamol, beclomethasone, or sodium cromoglycate [20]; IV clonidine [21]; IV dezocine [22]; a small pre-emptive dose of fentanyl [23]; or dilution and prolonged injection time [7]. We used nonpharmacological methods in our study to decrease the cost of treatment and hospitalization.
Yu et al. [7] studied the effects of dilution and prolonged injection time of fentanyl on FIC in 200 patients by diluting fentanyl to 50 µg/ml, 25 µg/ml, and 10 µg/ml with an injection time of 5 seconds and 10 µg/ml with a prolonged injection time of 30 seconds. The occurrence of cough was significantly reduced with the 10 µg/ml concentration and a 5 second injection time (12% versus 32% in the 50 µg/ml group), and a further reduced incidence was observed at 10 µg/ml with a prolonged injection time of 30 seconds (2% vs. 32%). They proposed that this phenomenon was due to the change in osmolality and pH of the fentanyl solution (caused by citrate in the fentanyl citrate solution) due to dilution with 0.9% normal saline. This change in osmolality and pH causes diminished stimulation of irritant receptors in tracheal smooth muscle and C fiber receptors in pulmonary vessels, thus preventing the cough reflex. In the present study, we found a lower incidence of FIC in the dilution group (6.8%) than in the control group (12.7%), but the difference was not statistically significant.
Acupressure has a role in anesthesia practice as documented by prevention of postoperative nausea and vomiting [2425]. The use of acupressure for prevention of acute cough in patients with asthma and chronic obstructive pulmonary disease is well documented in the literature [89]. There are five main acupressure points for cough relief: Heaven Rushing Out (CV 22, at the suprasternal notch), Elegant Mansion (K 27, below the medial ends of the clavicles on either side of the manubrium sterni), Heavenly Pillar (B 10, one-half inch below the base of the skull and one-half inch out from either side of the spine), Ding Chuan (Extra Point 17, to the side and just slightly above the vertebra that protrudes at the top of the spine when the head is tilted downward), and Vital Diaphragm (B 38, between the scapula and the spine at the level of the heart) [89]. Application of pressure to any of these points helps to relieve cough. Although the mechanism for prevention of cough by acupressure is not fully understood, it significantly reduces the incidence of FIC (1.3% vs. 12.7%, P = 0.008).
The limitation of our study was that our sample size was based on a 35% reported incidence of FIC in previous studies, but the actual incidence in our control group was 12.7%. Because of the lower incidence of FIC in our control group, our study may have been underpowered to detect a significant difference between the control and dilution groups and between the dilution and acupressure groups; a larger sample size would be beneficial to remove this bias. Another limitation is that all of our patients were female; the results of this study cannot be generalized to male patients.
In conclusion, the application of acupressure at the recommended points prior to administration of fentanyl significantly helps to reduce the incidence of FIC. Dilution of fentanyl also reduces the incidence of FIC, but this reduction is not statistically significant. The incidence of FIC in female patients in our cancer care institute is 12.7%.
 XML Download
XML Download