

 PDF
PDF Citation
Citation Print
Print



Oral endotracheal intubation is a routine procedure for patients requiring mechanical ventilation for general anesthesia. The main goal is to guarantee pulmonary gas exchange and protect the lungs against oral or gastric aspiration [1]. Difficult intubation scenarios complicated by laryngeal tracheal stenosis (LTS) can arise due to congenital factors or post-intubation injury, trauma, tracheal tumor, or compression of the trachea by a tumor. It is relatively rare, but the incidence of post-intubation tracheal stenosis is estimated at 4.9 cases per million per year [2], and primary diagnosis is often delayed until intubation is attempted.
Difficult intubation can occur even with comprehensive history taking and pre-anesthetic evaluations. Therefore, it is important to establish a detailed plan and preparation process for endotracheal intubation to avoid disastrous outcomes or unnecessarily invasive procedures. We report a case of failed intubation due to unanticipated post-intubation tracheal stenosis.
Case Report
A 69-year-old female patient (59.3 kg, 154.6 cm, body mass index 24.8) was scheduled for total knee replacement (TKR). Past medical history revealed that the patient underwent general anesthesia for prior TKR of the other knee three years at another hospital, and the patient failed to recall any specific events associated with anesthesia other than a sore throat, which is fairly common after intubation. The patient complained of occasional mild dyspnea during exercise, but chest radiographic readings by radiology were non-specific and we pursued further testing. Spirometry (FEV 2.27 liters (L), FEV1 1.84 L, FVC/FEV1 81%) and arterial blood gas analysis showed normal results. Both lung sounds were clear and no chest abnormalities were observed.
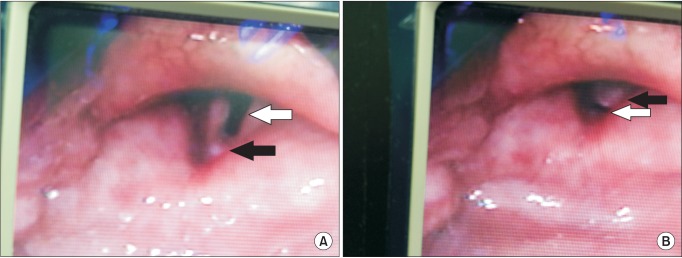
Upon entering the operating room, the patient was monitored with electrocardiograph electrodes, pulse oximeter, bispectral monitoring, and noninvasive blood pressure. After 3 minutes of pre-oxygenation with 100% oxygen, she was anesthetically induced with propofol (60 mg) and rocuronium (30 mg). After ventilating the lungs with a facial mask for two minutes without any difficulties, initial intubation was attempted with a conventional laryngoscope with the aim of inserting a 7.0 mm internal diameter endotracheal tube (ETT), which failed to pass the larynx. After a second attempt failed with a 6.5 mm internal diameter ETT due to continuous resistance when passing the vocal cords, we used a GlideScope® (Verathon Inc., Burnaby, Canada) to visualize and identify the source of the resistance. The GlideScope® view indicated that the subglottic area was divided into two sections with a septum (Fig. 1). A laryngeal mask airway (LMA, i-gel®, 4.0, Intersurgical Ltd., Wokingham, UK) was inserted for temporary ventilation with a tidal volume of 7 ml/kg and 12 breaths/min, but peak airway pressures of 30 mmHg did not improve even after injection of additional neuromuscular blockade. Predicting inadequate ventilation over several hours of anesthesia with i-gel® inevitably resulted in the attending anesthesiologist awakening the patient and postponing surgery until further evaluation. After reversing the neuromuscular blockade with sugammadex (Bridion®, MSD, Kenilworth, NJ, USA) 200 mg, the patient regained consciousness without any respiratory symptoms and the i-gel® was removed.
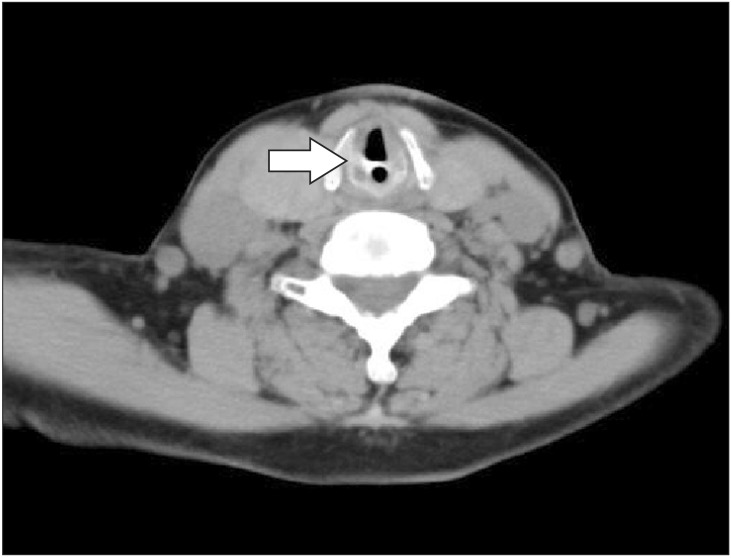
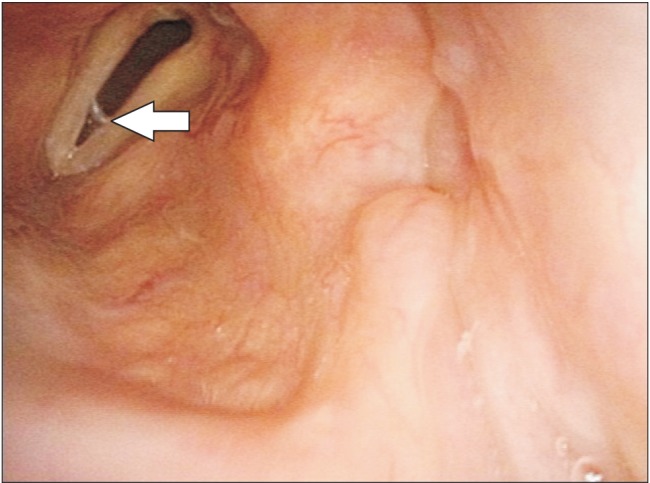
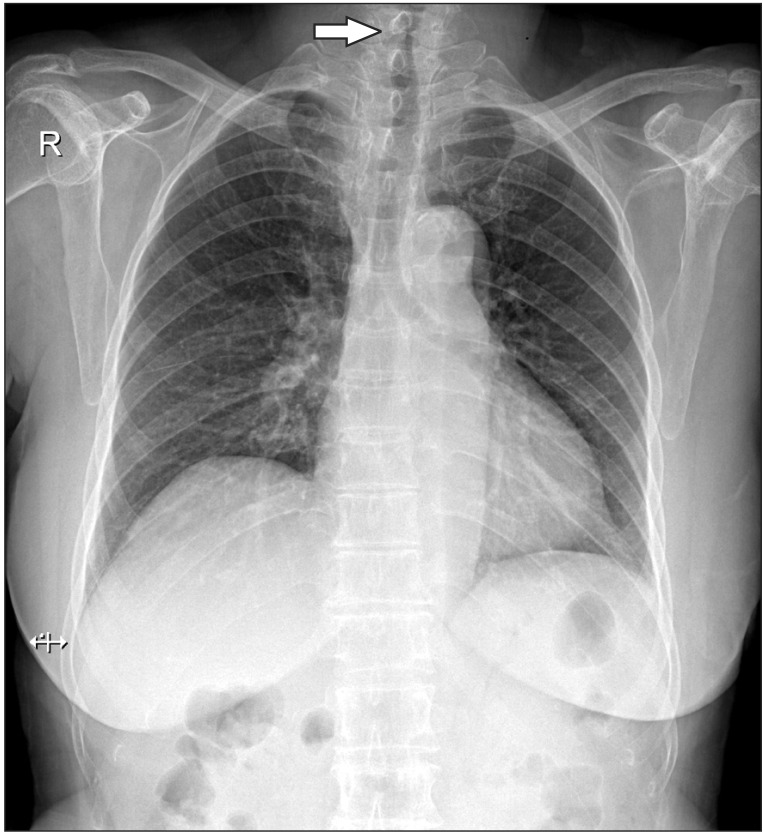
Neck computed tomography (Fig. 2) and fiberoptic endoscopy (Fig. 3) performed consecutively after surgery revealed fibrous tissue at the glottic level dividing the anterior and posterior portion into 5.8 mm and 1.7 mm lengths, respectively. An initial chest radiograph revealed evident narrowing at the level of the glottis (Fig. 4), with a post-anesthesia chest radiograph confirming the initial findings. Re-questioning the patient regarding any discomfort or complications from the previous surgery revealed that the patient suffered from severe dyspnea and dysphagia after surgery 3 years ago, which lasted several weeks. Afterwards, she complained of continuous mild dyspnea on exertion, but did not consider these symptoms to be anesthetic sequelae. An otorhinolaryngologist consulted for treatment diagnosed post-intubation tracheal stenosis, but did not recommend aggressive or invasive treatment. After constructing a plan including the use of a supraglottic airway (SGA) or smaller diameter ETT in case of failed regional anesthesia, the patient underwent successful surgery with continuous epidural block.
Discussion
Difficult intubations are challenging, even for vigilant anesthesiologists with years of experience. The main concern with difficult intubation or in cases where intubation fails is how to improvise methods for preventing such cases from becoming catastrophic before or during induction. Thus, providing safe anesthetic care and preventing intubation-related injuries remains a critical issue.
We first explored why preoperative tests such as chest radiographs, spirometry, and ABGA were unable to diagnose the tracheal stenosis. Because most patients remain asymptomatic until 30% of the original diameter becomes obstructed, medical history alone is insufficient in predicting difficult airways. Post-intubation tracheal stenosis may go unrecognized or even misdiagnosed as asthma [3] in patients whose symptoms are atypical. Thus, preoperative evaluations are essential in predicting difficult tracheal intubation, but with highly predicable tests currently lacking, only 50% of patients are actually found to have a difficult airway [4]. In addition, screening via methods such as Mallampati scores or measurement of thyromental distance lack reliability. A cohort study on the diagnostic accuracy of anesthesiologists in predicting difficult airways [5] claimed that 93% (3154 out of 3391 anticipated difficult intubations) were actually not difficult, calling into question the accuracy of the anesthesiologists' predictions and emphasizing the challenges that are constantly encountered during anesthetic preparation. Guidelines such as the difficult airway algorithm by the American Society of Anesthesiologists [6] provide strategies that ensure patient safety. In addition, Brichet et al. [7] have proposed a stepwise therapeutic algorithm for optimal management according to the severity of post-intubation tracheal stenosis.
In this case, we did not evaluate the airway tree upon the initial chest X-ray and relied solely on radiology interpretations. It may be challenging to differentiate true stenosis from vocal cord closure due to tracheal narrowing, or even C7 and T1 spinous process and lamina density without significant clinical symptoms or impressions. Therefore, more specific information regarding the patient's history may be useful for additional testing.
When encountering a patient with airway stenosis, an anesthesiologist would in general instinctively reattempt intubation with a narrower diameter ETT, but manipulation may compromise ventilation by increasing the risks of airway resistance, intubation failure, trauma, edema, bleeding, or perforation. However, the use of smaller ETT remains controversial due to the possibility of inadequate oxygen delivery and maintenance of ventilation from increased airway resistance and the work of breathing [8], and would not have been attempted. Even if this attempt had succeeded, potential airway edema and obstruction would have delayed extubation after observation in the intensive care unit. Positioning of the tube above or below the stenosis is also discouraged due to difficulties of proper fixation [9].
Despite known difficulties, ventilating patients with LTS is possible. Several cases of well-ventilated LTS have been reported. Donaldson and Michalek [10] inserted an i-gel® in a patient with no specific medical history other than having been informed to warn future anesthesiologists of her "small breathing pipe" as observed during her previous anesthesia. Furthermore, Lee et al. [11] ventilated a patient with a previous history of pulmonary tuberculosis and suspicious chest radiography findings in the beach-chair position with an i-gel®. Subglottic stenosis was visualized with a fiberscope through the i-gel® in both cases. Asai and Shingu [12] used a SGA and a tube-exchange catheter and inserted a reinforced 6.0 mm ETT in a patient undergoing surgery in the prone position. We believe that in our case, multiple attempts at intubation may have caused laryngeal edema, elevating peak inspiratory pressures which hindered ventilation with the use of i-gel®.
In our backup scenario, if continuous epidural anesthesia failed, intubation may have been attempted with a 5.5 mm ETT via a flexible fiberoptic bronchoscope (because the largest diameter between the septum measured 5.8 mm) and possibly fixed past the stenosis to avoid accidental extubation or tracheal damage. Intubation may also have been reattempted with a SGA.
Finally, preventable measures should be taken in daily practice to avoid factors causing LTS, such as high endotracheal cuff pressures exceeding 30 mmHg, which induce tracheal damage [13]. Perhaps choosing an ETT resistible to bending and collapse, with soft, thin-walled cuffs that are compliant, may be beneficial. Practitioners should also consider improvements in high-volume low-pressure cuffs by switching from standard polyvinylchloride cuffs to polyurethane cuffs [14] or the use of TaperGuard® tubes to decrease the length of cuff contact with the trachea and internal pressure, thereby reducing the incidence of compromised capillary perfusion resulting in tissue ischemia and proliferation [15]. At this time, because no clear recommendations or definite data indicate that one method is superior to the other, it may be best to adhere to the recommended internal cuff pressures and continuously check for over-inflation during surgery.
Endotracheal intubation may fail despite impeccable preanesthetic evaluation and preparations. However, with detailed history taking and comprehensive reevaluation, its cause can be determined. Anesthesiologists must always be prepared with anesthetic management plans that ensure patient safety in case of failure.
 XML Download
XML Download