

 PDF
PDF Citation
Citation Print
Print


Acute swelling of one or more of the parotid glands, commonly known as anesthesia mumps, is a clinical entity and one of rare complication following general anesthesia or even after epidural anesthesia [1]. When this phenomenon coexists with air and inflammation or infection, it is called pneumoparotitis. According to one report, the incidence of acute postoperative parotid swelling was 0.84% following a retrosigmoid and far-lateral skull base surgical approaches over a 4-year period [2]. As a complication of general anesthesia, anesthesia mumps had been reported in patients with obesity [3], in surgeries performed in the prone position [4], neurosurgical procedure [2], long-lasting surgery and sitting position [5]. While the exact mechanism and etiology has not been fully explained, it has been shown to develop in rare cases when the oral cavity pressure is increased by mask ventilation or by the coughing or sneezing of the patient and to be caused by air passing through Stensen's duct [3,4,5]. Some studies have reported self-induced pneumoparotitis via forced retrograde pneumatic auto-inflation by exhaling against a closed mouth or blowing to inflate a balloon [1,6]
We present a case of acute unilateral anesthesia mumps following usual positive-pressure face mask ventilation under general anesthesia without any predisposing factors.
Case Report
A 40-year-old, 165 cm tall, and 58 kg weighing female patient was diagnosed with a 6.7 × 9.3 cm sized uterine myoma. She was scheduled for hysteroscopic myomectomy under general anesthesia. Her physical status was American Society of Anesthesiologist class I. She had no specific medical history but morning stiffness, which was controlled with medication. The preoperative laboratory findings were within the normal range, including the white blood cell (WBC) count, which was 5,020 /mm3.
Upon arrival in the operating room, the patient's vital sign were blood pressure 120/60 mmHg, heart rate 78 beats/min, and oxygen saturation 98%. Electrocardiogram, pulse oximeter, capnogram, and noninvasive blood pressure were monitored. After preoxygenation with 100% oxygen, lidocaine 40 mg and propofol 120 mg were administered for the induction of anesthesia. Along with face mask ventilation, rocuronium 0.6 mg/kg was administered for muscle relaxation. Mask ventilation was continued for three minutes, and with airway pressure monitoring, the ventilation pressure was between 15 to 20 cmH2O. Following intubation, anesthesia was maintained with 50% oxygen and nitrous oxide and 6 vol% desflurane with controlled ventilation at end-tidal carbon dioxide around 30-35 mmHg.
The operation was performed for 30 minutes. At the end of surgery, glycopyrrolate 0.4 mg and pyridostgmine 10 mg were injected intravenously to reverse the muscle relaxation. With recover of spontaneous respiration, the patient was extubated, and mask ventilation was no longer necessary. She was observed for 30 minutes at the postanesthetic care unit, and then transferred to the general ward without any specific problem.
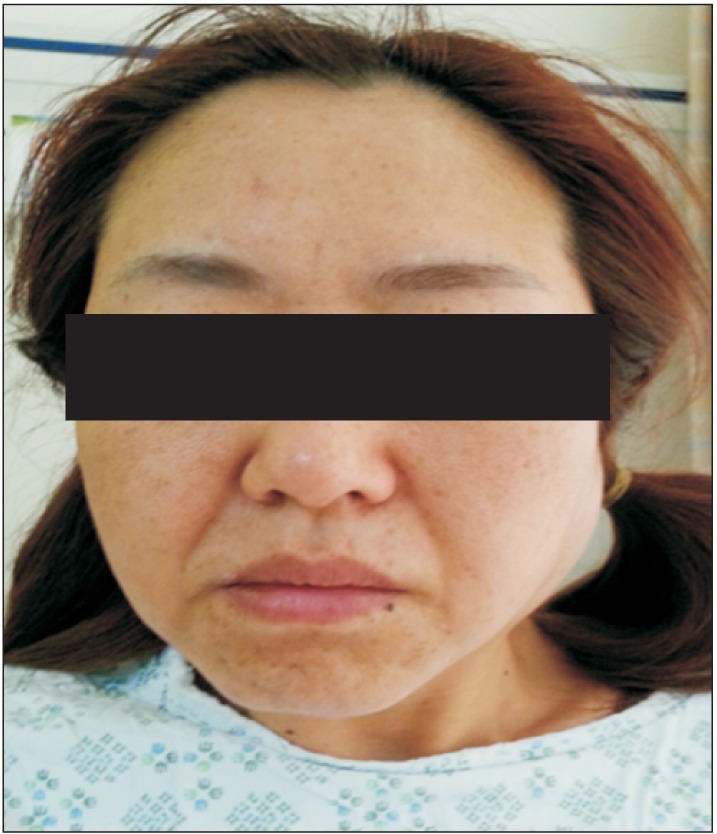
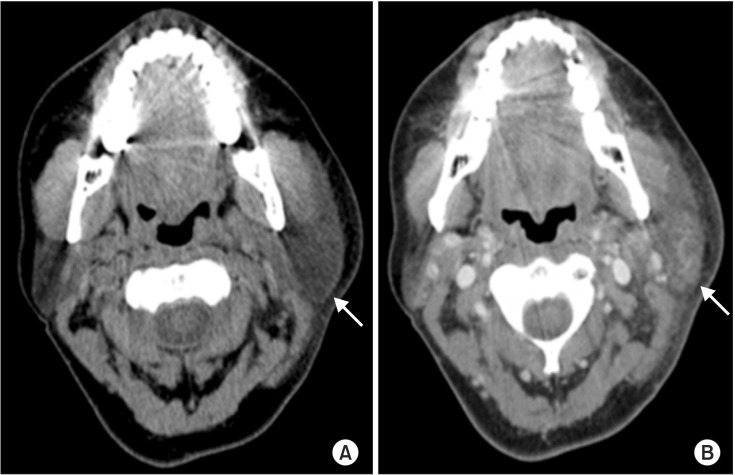
Thirty minutes after in the general ward, the patient complained of swelling in the left preauricular and submandibular triangle (Fig. 1) and pain with the visual analogue scale (VAS) 4. Diclofenac 75 mg was intramuscularly injected and an icebag was applied, so that the pain to decrease to VAS 2. Patient was consulted to an otolaryngologist. Oral examination revealed lingual edema and the presence of petechiae on the gums and the lateral border of the left cheek. Blood test results demonstrated inflammation with elevated WBC count 11,730 /mm3. We explained these results to the patient, and decided to evaluate more. Intravenous contrast-enhanced computed tomography (CT) of the neck demonstrated that left preauricular soft tissue swelling and enlargement and an enhanced left parotid gland with inflammation (Fig. 2). There were no abnormal findings in nasopharynx, oropharynx or airway below. To manage inflammation and to prevent bacterial infection, diclofenac 75 mg intramuscularly and cephalosporin 1 g were intravenously injected daily. Symptoms were persisted for 5 days, but progressively improved.
On the sixth day after the operation, she was discharged without complications.
Discussion
Acute swelling of the parotid gland after induction of general anesthesia is rare but can develop intraoperatively and in the immediate postoperative period up to 24 hours or even after discharge at home. This enlargement is tender with inflammation or infection and is called commonly anesthesia mumps. Other terms such as pneumoparotitis, parotitis, and pneumosialadenitis have been used in reports according to different causative factors but the clinical courses are similar. Numerous case reports of anesthesia mumps have been associated with a variety kind of surgeries including plastic, endoscopic, neurosurgical, abdominal, orthopedic, otolaryngologic, and a few types of gynecological procedures [5,7,8,9].
The exact mechanism of this anesthesia mumps is not yet fully understood, although several theories have been put forward. First, the loss of muscle tone induced during the general anesthetic procedure by muscle relaxants considered to be a factor. The flaccid musculature facilitates the retrograde passage of air into the parotid gland when the positive pressure in the oral cavity is significantly increased. And during emergence from general anesthesia, while a patient is still receiving positive pressure ventilation, excessive straining, coughing or sneezing can cause the retrograde flow of air through Stensen's duct, due to the loss of resistance in muscle tone around the orifice [4,6,7,8,9,10,11]. The result would be pneumoparotitis, a type of anesthesia mumps. However, there were no report mentioning the use of N2O that exaggerated the pneumoparotitis. Second, the retention of secretions can cause occlusion of the salivary ducts. Perioperative use of various drugs like glycopyrrolate, atropine, succinylcholine and morphine, as well as preoperative dehydration, can be also predisposing factors [3,9,12]. It is possible that activation of pharyngeal reflex which in turn simulates parasympathetic system that leading to hyperemia and vasodilation in the parotid gland [9]. Meanwhile, rebound vasoconstriction in the unblocked area of the epidural anesthesia possibly has an effect on parotid duct obstruction [1]. Third, anesthesia mumps can present in individuals undergoing dental treatment when the dentist is working near the molars or the angulation of the instruments is improper [13]. Fourth, the final possible explanation relates to the extremely rotated position of the patient's head during a long-lasting surgical procedure [2,4]. However, in our case, hysteroscopic surgery was performed in the lithotomy position, and the procedure lasted only a short time. Therefore, we thought positive-pressure mask ventilation as the most possible cause of anesthesia mumps in our patient, in addition to loss of resistance in muscle tone around Stensen's duct during general anesthesia. However, there was no air shadow in the lesion on the CT image, and duct obstruction by a reverse flow of air could be excluded. Another possibility is over pressure of mask fitting left hand which could temporally obstruct gland's orifices. We thought that lingual edema and bruise of gum on the left side could be a clue. That is, the mask holding finger pressure on the cheek overlying the duct or the patient's tongue or buccal mucosa bitten in the teeth can block the orifice of the glands during mask ventilation, similar to what happens in the dental procedure.
Various imaging studies, such as ultrasonography (US), sialography, radio-isotope scanning, CT, and magnetic resonance imaging have been used for diagnosis [10,12,14]. US may confirm subcutaneous emphysema with multiple hyperechoic areas within the affected side [6]. CT appears to be the best modality for the detection of small amounts of intra-parotid air because of its better resolution, faster acquisition, objectivity, and widespread availability. It usually demonstrates unilateral or bilateral swelling and edema, involving the parotid and submandibular gland, face, nasopharynx, oropharynx and hypopharynx. One clue in identifying pneumoparotitis from various causes of anesthesia mumps is crepitation on palpation.
Although several different mechanisms are suggested as above, clinical management is much the same. Some reports said that it can be resolved spontaneously within 48 hours [6,8], but others applied numerous management strategies from conservative care to surgical approaches [3,5,9,10,11,15]. Adequate hydration, mouth wash, pain control, and warm compresses on the affected side may be helpful [15]. Medical treatment such as oral or intravenous antibiotics can prevent secondary bacterial infection [9]. If the patient complains of severe or recurrent symptoms with infection and related complications, it may require surgical intervention like a Stensen's duct ligation or partial parotidectomy. In this case, symptoms were subsided with antibiotics and anti-inflammatory agent-Diclofenac and hydration.
To prevent the development of anesthesia mumps, many reports have suggested using adaptive-shaped soft pads conservatively and changing the head and neck position to avoid mechanical occlusion of the parotid gland and ducts [15]. However, in our case, anesthesia mumps developed after a short surgical procedure was performed in the lithotomy position without any predisposing condition. Therefore, the simple face mask fitting procedure to provied positive pressure ventilation could also play a part in parotid gland duct occlusion and swelling when it is done harshly. According to this conclusion, it is obvious that careful consideration should be given to patients with predisposing conditions like a long operation time, premedications involving anticholinergics, prone position, obesity, and a history of parotid disease or trauma. In addition, anesthesiologists should be aware that anesthesia mumps can develop with usual face mask handling, and a gentle procedure is always required.
 XML Download
XML Download