

 PDF
PDF Citation
Citation Print
Print


Endotracheal intubation is necessary in almost all cases of general anesthesia to maintain the airway. The endotracheal tube (ETT) sometimes causes airway obstruction secondary to secretions or other intraluminal materials, and it may cause hypoxemia and fatal outcomes [1,2]. We herein describe a case of a reversible ETT obstruction caused by meconium acting as a check valve, which was mistaken initially to be leakage from the anesthetic machine.
The patient was a 1-day-old male infant (height, 43 cm; weight, 1.7 kg). He was born by cesarean delivery at gestational age 34+3 weeks due to an omphalocele. The ruptured sac of the omphalocele (approximately 5 cm in diameter) was found at birth, and the emergency operation was planned. Before the surgery, he was already intubated because of meconium aspiration.
In the operating room, initial blood pressure and heart rate were 52/32 mmHg and 160/min, respectively, and SpO2 was 98%. A 3.0 mm uncuffed ETT had been placed at a depth of 8.5 cm, and a small amount of gas leakage was confirmed at the peak inflation pressure of 20 cmH2O. Both lungs were clear by auscultation, and no secretions drained from the ETT upon suction. The patient underwent pressure-controlled ventilation using the following settings: inspiratory pressure, 15 cmH2O; respiratory rate, 30/min; I : E ratio, 1 : 2. The tidal volume and end-tidal CO2 (ETCO2) were maintained at approximately 18-20 ml and 32-35 mmHg, respectively. SpO2 was maintained at > 95% during the operation.
The surgeon repaired the entire intestine and began to close the abdominal cavity 3 hours after the surgical incision. Capnography showed an obstructive pattern, and ETCO2 increased slightly to 38-40 mmHg with no change in ventilator settings. We suctioned the ETT again using a 6-Fr suction tip, and there was no resistance or secretion.
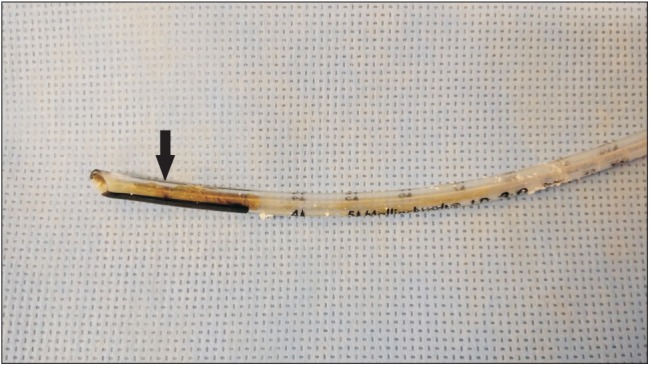
Upon completion of the abdominal closure, the surgeon decided to place an internal jugular venous catheter for postoperative care. The ventilator leakage alarm sounded during venous cut-down. The tidal volume decreased from 20 to 5-7 ml, and ETCO2 decreased to < 10 mmHg. The capnography curve exhibited a blunt concave slope during the expiratory phase. The ETT was confirmed to be positioned correctly, and there was little gas leakage around the ETT. A full examination of the anesthetic machine and breathing circuit, including capnography, revealed no abnormalities, but the SpO2 had decreased to 88%. Upon switching to manual ventilation during examination, we encountered resistance during the inspiratory phase. Chest auscultation revealed inspiratory rales and faint expiratory wheezing in both lung fields. The ETT suction was repeated, but no secretion was seen. The ETT was removed, and we reintubated with another 3.0 mm uncuffed ETT under direct laryngoscopy. The tidal volume was 20-25 ml at an inspiratory pressure of 15 cmH2O, and capnography showed a normal plot. The ETCO2 measured immediately after reintubation was 58 mmHg and decreased to 33-35 mmHg after hyperventilation for 3 minutes. Inspection of the removed ETT revealed thick meconium approximately 2 cm long plugging the distal lumen of the ETT. Additionally, an approximately 0.3 cm-long inspissated meconium was dangling from the superior portion of the inner wall of the ETT (Fig. 1).
ETT obstruction due to bronchial secretions is usually suspected by abnormally high peak inspiratory pressures, a significant difference between the measured inhaled and exhaled tidal volumes, decreased lung compliance, increased resistance to inflation, and an obstructive pattern on capnography [3]. In the present case, the peak inspiratory pressure was constant because the pressure-controlled mode was set. The concave capnography plot with a low expiratory tidal volume caused the ETT obstruction to appear as a leak in the anesthetic machine. We initially suspected the leak around the ETT, because the patient's head was rotated for preparation of venous catheterization and there was the possibility of movement of the ETT. We also suspected leakage of the breathing circuit according to the capnography results, because sidestream devices typically extract a sample of gas of 50-200 ml/min, and the sampling volume often exceeds the fresh gas flow and causes anesthetic machine leaks in small pediatrics [4]. However, no ETT movement or leakage was confirmed, and no leak occurred at the same ventilation settings for more than 3 hours. Because in our pursuit of the cause, we were concerned only with the leak, the obstruction was identified belatedly.
Based on the inspection of the first ETT, the proposed sequence of events is as follows. The dangling meconium might have allowed for inspiration because positive-pressure ventilation was administered. After the termination of inspiration, the dangling meconium might have obstructed the lumen of the ETT and acted as a one-way check valve, preventing minimal gas egress. As a result, the expiratory tidal volume might have decreased, and a flow sensor in the expiratory limb must have detected this change as a leak in the anesthetic machine. Use of the pressure-controlled mode interrupted the early diagnosis of airway obstruction, but fortunately prevented an excessive increase in the intrathoracic pressure in the lung without a way to relieve it.
We used a heated breathing circuit with a humidifier in this case. However, the humidified inspiratory gas did not entirely prevent accumulation of meconium in the ETT, despite the fact that it may have induced slow accumulation. It was possible that the ETT obstruction occurred by the upward movement of meconium in the lower airway, as indicated by the changing shape of the capnography curve upon closure of the abdominal cavity. Moreover, the suction catheter may not have been inserted to a sufficient depth to reach the meconium, or the suction catheter that fit the small lumen of the ETT was too thin to remove the thick meconium. More meconium accumulated with time, and the dangling meconium may have acted as a check valve.
In conclusion, anesthesiologists should consider the possibility of delayed airway obstruction in meconium-stained babies. Frequent and sufficient suction must be performed in these patients. Additionally, when the leakage alarm of the anesthetic machine sounds, we suggest that the anesthesiologists consider the possibility of the plugged material acting as a check valve.
 XML Download
XML Download