

 PDF
PDF Citation
Citation Print
Print


A central venous catheter (CVC) can be placed through various veins according to the clinician's preference, the indication for catheterization, and the patient's medical condition [1]. The right internal jugular vein (IJV) has been the preferred site for central venous cannulation because it is easy to insert a CVC at this location by using the anatomical landmarks of the internal carotid artery (ICA) and the sternocleidomastoid muscle (SCM) [1]. In addition, the right IJV follows a short and straight path to the superior vena cava (SVC), allowing easier placement of the CVC in the SVC and a slim chance of misplacing the CVC into the wrong vessels [1,2]. Despite these advantages of the right IJV, we experienced a case of misplacing a CVC into the wrong vein, mistaking it for the IJV. Therefore, we report this case along with a review of the literature.
Case Report
A 65-year-old male, with a body mass index of 30 kg/m2 (163 cm, 80 kg), was admitted with dyspnea on exertion. The patient was scheduled for a coronary artery bypass graft for treatment of angina pectoris. His past medical history included hypertension, diabetes mellitus, and cerebral infarction. Preoperative electrocardiogram showed first-degree atrioventricular block, but there were no other abnormalities on preoperative examination.
The patient's vital signs after arrival in the operating room were blood pressure (BP) 140/70 mmHg, heart rate (HR) 70 beats/min, and oxygen saturation (SpO2) 100%. An arterial catheter was inserted via the left radial artery for continuous BP monitoring. Anesthesia was induced with intravenous etomidate 14 mg, rocuronium 50 mg, and fentanyl 200 ug.
The patient's head was rotated leftward 20-30° in head-down position for insertion of a triple-lumen 7-Fr CVC (Bioline, Ewha Biomedics, Seoul, Korea) via the right IJV, but the anatomical landmarks were not clearly distinguished. After additional rotation of the head to 30°, the triangle consisting of the two heads of the SCM muscle and the clavicle was recognized and the pulsation of the ICA was felt from the superior angle of this triangle. A 23 G finder needle was inserted at a 30° angle in the site where both bellies of the SCM joined and the pulsation of the ICA was about 0.5 cm distinct, and was advanced toward the ipsilateral nipple. Non-pulsatile blood was aspirated at a depth of 3.0 cm. After removal of the finder needle, an 18 G puncture needle was inserted in the same direction, but venous blood was not aspirated at a depth of over 4.0 cm. Under the presumption that the thick puncture needle might lead to a collapsed IJV, the needle was drawn back while aspirating. Immediately after the needle was pulled back, non-pulsatile dark-colored blood flow was observed. As the J-tipped guide wire was advanced to 25 cm from the skin surface, the ECG monitor showed arrhythmia, and the wire was withdrawn about 5 cm. The CVC was then inserted and fixed at 14 cm after confirming free regurgitation of blood. Central venous pressure (CVP) was measured to be 9 or 10 mmHg, and the withdrawn wire had no deformities. A chest X-ray was performed to confirm the location of the CVC.
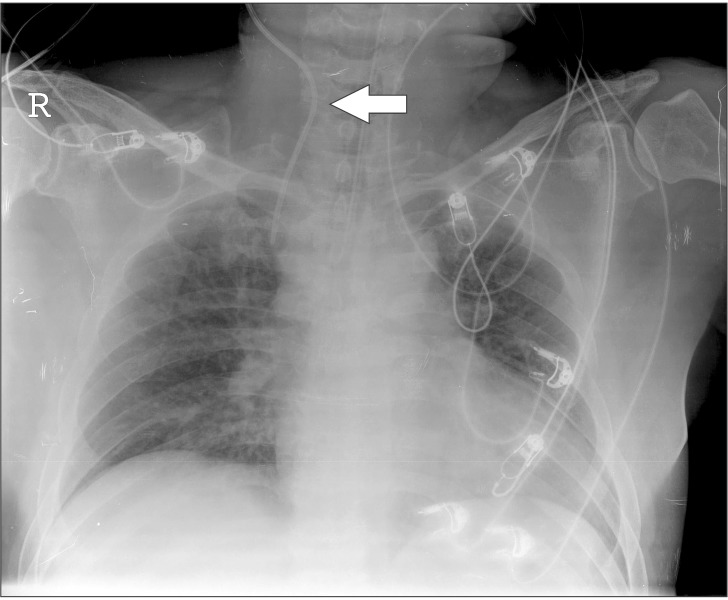
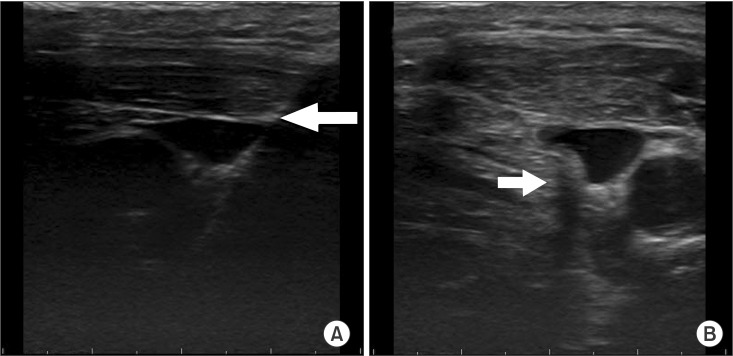
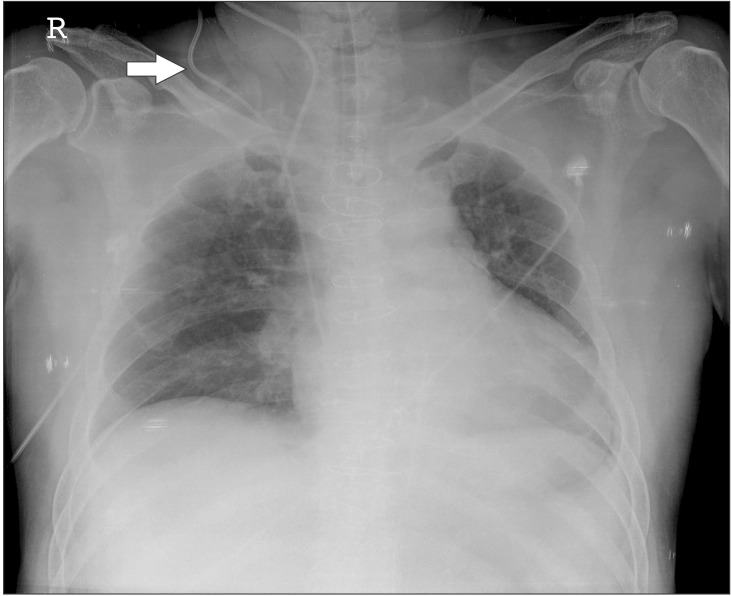
According to the radiologist's reading of the chest X-ray, the CVC passed the transverse processes of the 6th and 7th cervical vertebrae (Fig. 1). Longitudinal view from the ultrasound (according to the course of the CVC) showed that the catheter was closely passing the right wall of the IJV and proceeding deep (Fig. 2A). However, the exact location of the catheter tip could not be identified. Axial view of the IJV showed that the catheter shadow was located not in the vein but in the deeper posterior part (Fig. 2B). The catheter was placed in neither the ipsilateral ICA nor the subclavian vein. Taking the ultrasound and chest X-ray into consideration, it was presumed that the CVC had been inserted into a vein other than the IJV. A new catheter was placed in the right subclavian vein under ultrasound guidance. Longitudinal view showed that the catheter proceeded along the right subclavian vein. Tip position in the SVC was confirmed by transesophageal ultrasound. The misplaced catheter was maintained along with the newly inserted CVC during the surgery (Fig. 3), due to the possibility of hemorrhage induced by intraoperative heparin administration. The operation was performed with no complications.
Following the surgery, the patient was transferred to the intensive care unit. The bleeding from the surgical site was minimal, and the activated clotting time was 119 seconds. The misplaced catheter was removed. Physical examination revealed no hematoma or bruit at the puncture site after 15 minutes of compression. The patient was extubated the following day and transferred to the general ward. He did not experience any neurologic symptoms and was discharged on the 14th day after the operation.
Discussion
In this report, we attempted to place a CVC in the right IJV by using anatomical landmarks, and observed free regurgitation of non-pulsatile blood flow and normal central venous pressure (9-10 mmHg). However, ultrasound showed that the catheter was placed outside the lumen of the IJV, and was advancing backward. The CVC was nowhere to be observed in the ICA, IJV, or subclavian vein. All things considered, it was suspected that the CVC was placed in some vein situated posterior to the IJV.
Notable veins surrounding the IJV are the vertebral vein, the external jugular vein, the anterior jugular vein, and the thyroid vein [3]. The only vein passing posterior to the IJV is the vertebral vein [3]. The vertebral vein passes through the transverse foramina from the atlas to the 6th cervical vertebra [3,4]. After exiting the transverse foramen of the 6th vertebra, it subsequently subsequently runs anterolateral to the vertebral artery and posterior to the IJV and drains the innominate vein [3,4]. In this case, ultrasound revealed that the location of the inserted catheter was posterior to the IJV (Fig. 2B). Chest X-ray also showed that the catheter passed the transverse processes of the 6th and 7th cervical vertebrae, running toward the innominate vein (Fig. 1). Therefore, the inserted CVC had a course very similar to that of the vertebral vein. A case was previously reported in which the CVC was inserted via the vertebral vein [5]. The CT scan in that case showed identical placement of the catheter to that revealed by the chest X-ray in our case [5]. Puncture of the vertebral artery adjacent to the vertebral vein is well known to occur as a complication of CVC insertion via the IJV [6]. Puncture of the vertebral vein is quite rare, but it does happen [5,7]. In addition, the vertebral vein has a cross-sectional area of 10.6-11.9 mm2 [8], and we suppose that CVC insertion via the vertebral vein is sufficiently possible. These pieces of evidence support our hypothesis that the vein in which the catheter was placed in this case was the vertebral vein, not the IJV.
Failure to puncture the IJV and the insertion of the CVC through the vertebral vein could result from excessive rotation of the patient's head. Leftward rotation of the patient's head may cause the right IJV to overlie the ICA [1,9], thereby increasing the probability of failure to puncture the IJV and of puncturing the vertebral vein just behind the IJV. Therefore it has been recommended to minimize the head rotation, not exceeding 30° [9,10]. In this case, excessive leftward rotation of the head to improve recognition of surface landmarks altered the anatomy of the IJV and may have led to failure to puncture the IJV.
Advancing the puncture needle to a depth of more than 4 cm could also have been a cause for the vertebral vein puncture in this case. The patient was obese, with BMI 30 kg/m2, leading to the assumption that the distance from the skin surface to the IJV could be greater than that in a non-obese patient. Therefore, the needle was inserted deeper than usual. A previous report, however, showed that the maximal distance from skin to the IJV rarely exceeded 3.5 cm if the needle was inserted at a 30° angle to the skin surface [9]. Therefore, inserting the needle more than 4 cm seemed to be an excessive approach. It is more effective in obese patients to use ultrasound because obesity may limit the identification of anatomical landmarks. It has been reported that ultrasound-assisted access of the IJV in CVC insertion significantly improved success rates, decreased the time necessary to complete the procedure, and reduced the frequency of complications [11,12].
Arterial puncture, the most common complication of CVC insertion, is distinguished with comparative ease. However, the misinsertion of the catheter into other veins instead of the IJV cannot be easily distinguished from a successful CVC insertion because it is a rare occurrence, and there is no difference in the color and pulsation of the regurgitated blood flow. Catheter misplacement into a small vein such as the vertebral vein increases the possibility of complications, including trapping of the catheter, thrombosis, endothelial damage, and leakage of infused fluid [6]. It is also not possible to deliver hypertonic or hyperosmolar solutions [6]. Therefore, it is necessary to confirem the location of the catheter after insertion of the CVC. In addition, if the CVC is found to have been misplaced in a small vein, as in this case, the reinsertion of a new CVC in a different proper vein seems to be appropriate despite free regurgitated blood flow from the misplaced CVC.
Plain chest radiograph has been considered the gold standard for confirming the location of the catheter tip [1]. However, this method has a limited ability to assess the true position of the CVC because it is a two-dimensional image [13]. Therefore, it may not be possible to identify whether the catheter is placed in the SVC or, anterior or posterior to the SVC from a plain chest radiograph. Ultrasound is also a diagnostic tool for catheter misplacement [14]. It can show in real time when the catheter is inserted in the subclavian vein and the IJV during central venous catheterization. However, transesophageal ultrasound is needed to confirm the position of the catheter tip in the SVC [13], and this requires time, trained manpower, and special equipment. The two methods obviously have their own advantages and disadvantages. Thus, clinicians need to know the limitations of each method when plain radiography or ultrasound is used to confirm the position of a CVC.
In conclusion, it is necessary to confirm the placement of a CVC with a radiograph or ultrasound. When the course of a catheter passes close to the transverse process of the 6th cervical vertebra, placement of the CVC in the vertebral vein should be considered. The misplacement of a CVC into the vertebral vein might occur from excessive rotation of the head, which leads to alterations in the cervical vascular anatomy, and from deep insertion of a puncture needle. Therefore, it is advised, for safe CVC insertion, to minimize a patient's head rotation and the insertion depth of a puncture needle, and to make use of ultrasound when the anatomical structures cannot be clearly identified.
 XML Download
XML Download