

 PDF
PDF Citation
Citation Print
Print


Introduction
Coughing caused by irritation from an endotracheal tube frequently occurs during emergence from general anesthesia, and the incidence of cough is reported from 38 to 96% [1-3]. Such coughing can cause hypertension, tachyarrhythmia and various complications can occur including a subsequent increase in intracranial pressure, bleeding in the operated site, and disruption of surgical wounds from excessive movement [4,5]. Various methods have been studied to prevent coughing during emergence from general anesthesia, such as extubation in a deep plane of anesthesia [6], intra-cuff application of lidocaine [1] or i.v. lidocaine [7], and administration of dexmedetomidine [8] and remifentanil [9,10]. These methods have various advantages, but they also have drawbacks so their clinical use can be limited.
Propofol is used widely in clinical anesthesia, and it is known to be an inhibitor of airway reflexes [11]. Recently, there have been reports that patients who received total intravenous anesthesia (TIVA) using propofol showed less prevalence of coughing during emergence compared to patients who received balanced anesthesia (BAL) using sevoflurane [12,13]. In addition, it has been reported that single i.v. administration of a subhypnotic dose of propofol effectively prevented laryngospasm and coughing during emergence in children [14,15]. However, there are no studies yet on the effect of administering a subhypnotic dose of propofol for coughing and on the recovery time during emergence in adults who were anesthetized with sevoflurane and remifentanil.
Therefore, this study was conducted to examine whether single administration of a subhypnotic dose of propofol can reduce the incidence and severity of coughing in adults during emergence from general anesthesia when using sevoflurane and remifentanil. In addition, the effect of propofol administration on the recovery time and hemodynamics of adults was examined.
Materials and Methods
This study was approved by the Institutional Ethics Committee, and written informed consent was obtained from the patients. Among patients who were scheduled for elective nasal surgery under general anesthesia, 60 patients of American Society of Anesthesiologists physical status I-II and age 18-65 were chosen as subjects. Patients with anticipated difficulty in endotracheal intubation, and patients with mental, neurologic, cardiovascular, lung, or kidney disease were excluded as research subjects. In addition, in the pre-operative visit, patients wearing hearing aids due to some hearing disturbance or unable to have conversations in a normal voice were excluded as study subjects.
Using computer-generated random numbers, the patients were divided into two groups according to the administration of propofol or normal saline. Propofol 0.3 mg/kg for the propofol group (n = 30) and normal saline 0.03 ml/kg for the control group (n = 30) were prepared at the completion of the surgery by the authors who did not participate in the anesthesia, and the syringes were wrapped with white tape to hide the color difference between the study drugs.
All patients fasted for 8 hours before the operation, and were premedicated with i.m. midazolam 2.5 mg before induction. Upon arrival in the operating room, electrocardiogram, non-invasive blood pressure (Philips MP40), pulse oximeter, bispectral index (BIS) (BIS™ quarto, Covidien, Mansfield, MA, USA), and tympanic thermometer were used to monitor vital sign and BIS value.
Before induction, lactated Ringer's solution 5 ml/kg was administered for 5 minutes and preoxygenation was conducted with 100% oxygen. After i.v. administrating glycopyrrolate 0.2 mg, remifentanil 0.5 µg/kg and propofol 1.5 mg/kg were i.v. administered to induce anesthesia. Rocuronium 0.8 mg/kg was i.v. administrated to induce muscle relaxation, and endotracheal intubation was conducted using endotracheal tube with an internal diameter of 8.0 mm for males and 7.0 mm for females. Then a hand pressure gauge (Hi-Lo™ Hand Pressure Gauge, VBM Medizintechnik GmbH, Sulz a.N., Baden-Württemberg, Germany) was used to fill with air until the cuff pressure reached 20-25 mmHg, and the pressure was maintained at 20-25 mmHg until the surgery ended. Anesthesia was maintained with continuous infusion of remifentanil 0.05-0.20 µg/kg/min and sevoflurane 1.5-2.5%. Throughout the surgery, depth of anesthesia was titrated to maintain a BIS value between 45 and 65, and the mean arterial pressure (MAP) and heart rate (HR) were maintained within ± 20% of the pre-induction values. Mechanical ventilation was controlled to maintain the ETCO2 at 30-35 mmHg, and the temperature was maintained at 36-37℃.
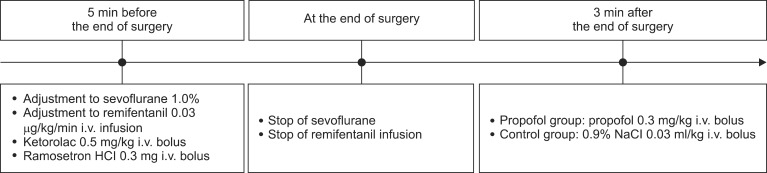
Two anesthesiologists who were unaware of the patient groups participated during the emergence phase. The entire procedure from anesthesia induction to emergence was conducted by a skilled anesthesiologist, and measurements such as MAP, occurrence of coughing, and severity of coughing were recorded by another anesthesiologist. Five minutes before the end of surgery, the concentration of sevoflurane was adjusted to 1.0% and remifentanil to 0.03 µg/kg/min for both groups until the end of surgery. In addition, ketorolac 0.5 mg/kg was administered for postoperative pain control, and ramosetron HCl 0.3 mg to reduce postoperative nausea and vomiting.
After the completion of surgery, blood and secretions in the oral cavity were gently suctioned, and sevoflurane and remifentanil were discontinued. Afterwards, mechanical ventilation was discontinued while manual ventilation was performed with 5 L/min oxygen. When train-of-four response was measured at 90% or more, glycopyrrolate 8 µg/kg and pyridostigmine 0.2 mg/kg were i.v. administered to reverse the residual neuromuscular blockade. Three minutes after discontinuing sevoflurane and remifentanil, a nurse who was unaware of the patient groups i.v. injected the previously prepared study drugs for 10 seconds (propofol 0.3 mg/kg for the propofol group and normal saline 0.03 ml/kg for the control group) (Fig. 1).
Extubation of the endotracheal tube was performed when the patient followed oral commands of "Open your eyes" and showed regular spontaneous respiration, or when the patient attempted self-extubation. Five minutes after extubation, the patients were transported to the post-anesthesia care unit (PACU).
The time taken from discontinuing the anesthesia to opening the eyes in response to oral command, and to extubation was recorded. Occurrence and grade of coughing were measured in the operating room from the discontinuation of anesthetic drugs to 5 min after extubation. The grade of coughing was measured in 4 grades, where an additional no cough grade was added to the 3-grade scale used in the study of Minogue et al. [16] (Grade 0; no cough, Grade 1; single cough, Grade 2; more than one episode of unsustained [≤ 5 s] coughing, Grade 3; sustained [> 5 s] bouts of coughing).
The BIS value was measured at the point of discontinuing the anesthetic drug, immediately before and after extubation, 5 minutes after extubation, and 10 minutes after PACU. At the time points of 5 minutes after extubation and 10 minutes after PACU, the grade of sedation was additionally measured according to the following grading system used by Lee et al. [9]: Grade 0 was deep sedation where there was no response to a loud voice calling the patient's name and "Open your eyes"; Grade 1 was when the patient was sedated but opened their eyes when called in a loud voice; Grade 2 was when the patient was sedated but opened their eyes when called in a normal voice, and Grade 3 was when the patient opened their eyes and showed a response.
MAP and HR were measured before induction, at the discontinuation of the anesthetic drugs, immediately before and after extubation, 5 minutes after extubation, and 10 minutes after PACU. In addition, while in the PACU, occurrence of respiratory depression, headache, dizziness or nausea, vomiting, discomfort such as pain of VAS 5 or more, and complications were recorded.
The sample size was determined by referring previous studies which reported that the incidence of coughing after general anesthesia was 76% [3]. When it was hypothesized that using propofol would reduce the occurrence of coughing to 50%, 25 patients are needed per group for a power analysis of 0.8 (α = 0.05, β = 0.2). Here, in anticipation of dropout, 30 patients per group, 60 patients in total, was determined.
PASW Statistics 18.0 software (SPSS Inc, Chicago, IL, USA) was used for all statistical analyses. To test the normality of the distribution of the continuous variables, the Shapiro-Wilk test was done. The normally distributed data were compared between the groups with two-tailed unpaired, Student's t-test and expressed as the mean ± SD. Non-normally distributed variables were evaluated with the Mann-Whitey U test and expressed as the median and interquartile range. The categorical data were analyzed with the Chi-square test or the Fisher's exact test as appropriate. The repeated-measures analysis of variance was used for evaluated the change in MAP, HR, and BIS between the groups according to time. Results were considered to be statistically significant when the P value was less than 0.05.
Results
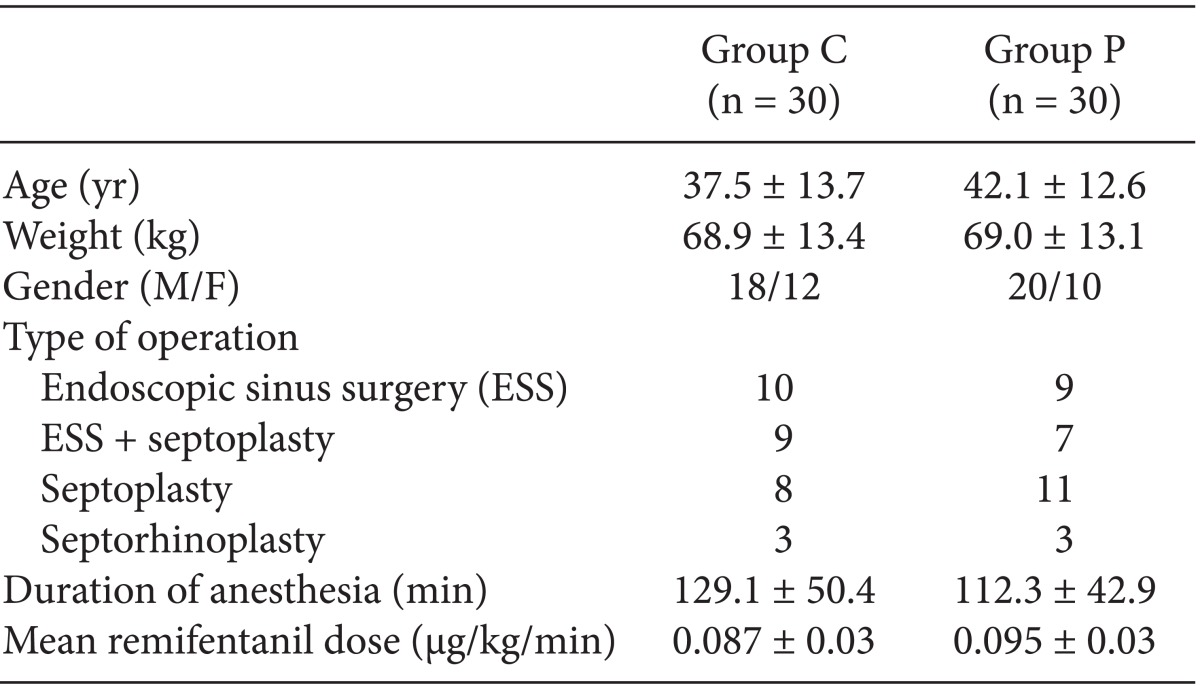
There were no differences between the groups in demographic characteristics, type of surgery, duration of anesthesia, and mean remifentanil dose (Table 1).
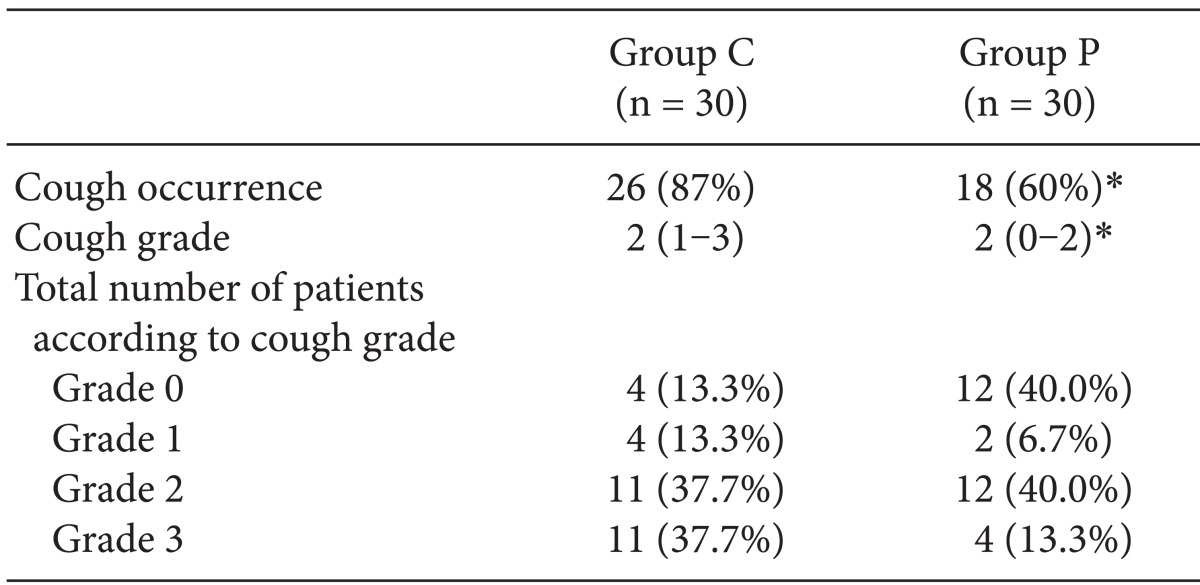
The incidence of coughing during emergence was significantly lower in the propofol group compared to the control group (60 vs 87%, P = 0.04). The grade of coughing during emergence was also significantly lower in the propofol group than in the control group (P = 0.02) (Table 2).
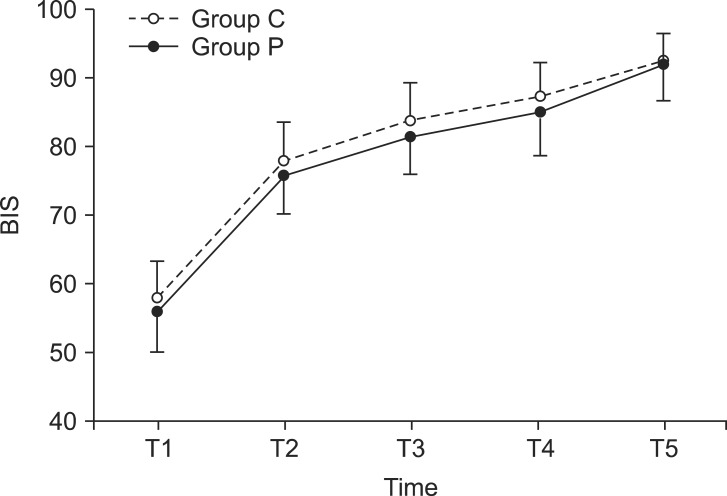
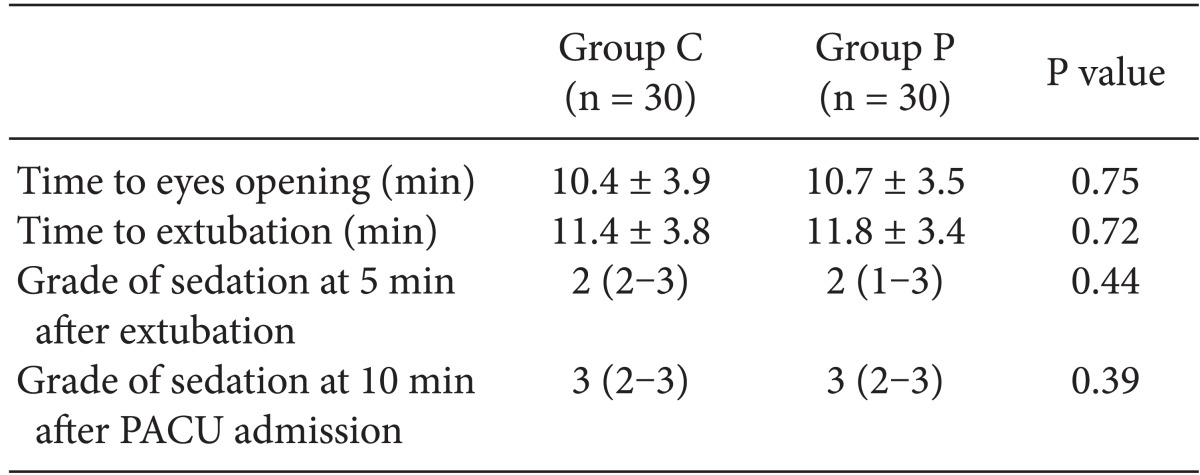
The time period from the discontinuation of the anesthetic drugs to opening of the eyes was 10.6 ± 3.5 minutes in the propofol group and 10.4 ± 3.9 minutes in the control group. The time taken until extubation for the propofol group was 11.8 ± 3.4 minutes and 11.4 ± 3.8 minutes for the control group, so there were no statistically significant differences. There was also no difference in the grade of sedation between the groups at 5 minutes after extubation and 10 minutes after PACU (Table 3). The BIS value at the discontinuation of the anesthetic drugs also did not show a significant difference between the groups (P = 0.25). There were also no differences between the two groups in the subsequent changes according to time (P = 0.85) (Fig. 2).
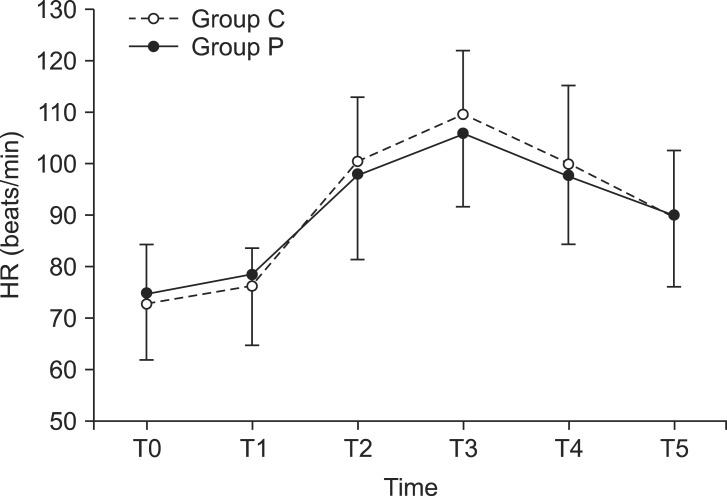
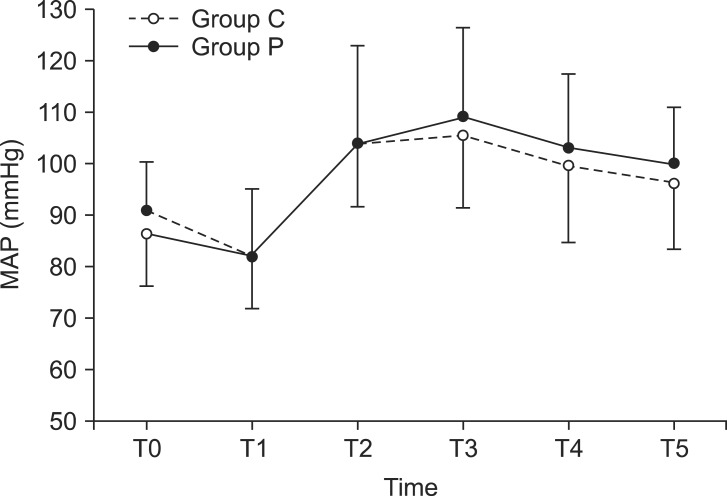
The HR and MAP before induction did not show a significant difference between the two groups (P = 0.53, 0.10). The subsequent change in HR according to time during emergence was also not significantly different between the two groups (P = 0.23) (Fig. 3). There was also no significant difference between the groups for change in MAP according to time during emergence (P = 0.22) (Fig. 4).
In the PACU, 1 patient in the control group complained of pain with a VAS score of 5, so fentanyl 50 µg, was i.v. administered and there were no such cases in the propofol group. Complications such as respiratory depression, headache, dizziness, nausea, and vomiting did not occur in both groups.
Discussion
In this study, patients who underwent nasal surgery with anesthesia maintained by sevoflurane and remifentanil had significantly reduced an incidence and severity of coughing during emergence without extending the recovery time, when a single dose of propofol 0.3 mg/kg was administered 3 minutes after discontinuing anesthetic drugs. Such results are similar to a report that the incidence of coughing was reduced in children when propofol 0.25 mg/kg was used 1 minute before extubation (53 vs 83%, P = 0.047) [15].
Coughing during emergence is caused by activation of the sensitive ascending vagus nerve distributed in the airway from chemical and mechanical irritation [17]. Additionally, it is known that other ascending nerve subtypes and visceral organ, chest wall, diaphragm, and abdominal muscles controlled by the nerve also play an important role in the occurrence of coughing [18]. Propofol reduces the reflexes of the larynx and airway in proportion to the amount used [11], and such an effect can appear further accelerated when used together with opioids [19]. In addition, the effect of propofol on the central nervous system is to enhance the γ-aminobutyrateA (GABA) induced chloride current through its binding to the GABA A receptor [20]. In addition, propofol controls sodium channel gating and subsequently inhibits the N-methyl-D-aspartate (NMDA) subtype of the glutamate receptor [21]. There are reports that the occurrence of coughing was reduced when NMDA receptors were blocked [22,23], so the inhibition of NMDA receptors by propofol may have reduced the occurrence of coughing. However, in children, propofol had a better effect in the suppression of coughing during emergence than that of ketamine known as the representative NMDA antagonist [15]. Considering these points, the NMDA inhibition effect of propofol is less likely to be the main mechanism for supressing coughing, and there is need for more clinical studies regarding this matter.
A single i.v. injection of propofol during emergence is usually used in children to reduce laryngospasm and emergence agitation [14,15,24], but there have been no reports yet on the effect of a subhypnotic dose of propofol during emergence on coughing and the recovery profile of adults whose anesthesia was maintained with sevoflurane and remifentanil. Therefore, to obtain the desired effect of propofol in adults during emergence, the administration dosage and time have to be determined carefully. Aouad et al. [24] reported that emergence agitation was reduced in children when a single dose of propofol 1.0 mg/kg was administered at the end of surgery, but the recovery time was significantly delayed around 4 minutes compared to when propofol was not administered. In addition, Cohen et al. [25] reported that when propofol 2 mg/kg was administered in addition to inhalation anesthesia in children before the start of surgery, it did not reduce emergence agitation. This result can be because the effect of propofol administered at the start of surgery was not continued until emergence. Our research referred to previous studies which reported that it took approximately 7.2-12 minutes from the time of discontinuing anesthetic drugs to extubation when anesthesia had been maintained with sevoflurane and remifentanil [12,13]. Accordingly, the authors decided to administer 0.3 mg/kg of propofol as a single dose 3 minutes after discontinuing the anesthetic drugs. The dosage was a 10 minute-dose of the continuous infusion rate, which was 30 µg/kg/min, needed for the hypnotic effect-the effective dosage ranged from 30 to 60 µg/kg/min [26]. In our study, there were no patients who showed an emergence response before administering the propofol, which was in 3 minutes after discontinuing the anesthetic drugs. The time taken for eye-opening and extubation was 20 seconds longer in the propofol group compared to the control group. However this was not statistically significant. Although a direct comparison is difficult because the pharmacodynamics of propofol is different in adults and children [27], the dosage of propofol used in this study was smaller (0.3 mg/kg) than the amount used in the study on children (1.0 mg/kg) [24]. Therefore, we think that there was less effect on delaying emergence.
In our study, the BIS value showed a slight decline immediately after administering propofol, but the BIS value was similar to the control group at the time of eye opening, extubation, 5 minutes after extubation, and 10 minutes after PACU. In addition, most of the propofol group were awake or opened their eyes in response to a normal voice at 5 minutes after extubation, and at 10 minutes after PACU. At both time points, there was no difference compared to the control group. However, there were 2 patients in the propofol group who showed sedation of Grade 1, where they did not respond to a normal voice but responded to a loud voice, at 5 minutes after extubation, while all the patients in the control group were Grade 2 or higher where they responded even to a normal voice. Although no patient showed respiratory depression in our study, the effect of sedation appeared differently even for propofol 0.3 mg/kg due to individual differences. Therefore, when administrating propofol during emergence, there is a need for careful monitoring taking into consideration the sedation of patients when transported to PACU.
Propofol can significantly decrease the arterial pressure according to the dosage used during anesthetic induction [28,29], and this appears in relation to systemic vascular resistance and a decrease in cardiac output. In addition, it does not have a significant direct effect on HR, but it may increase [30]. In our study, the MAP and HR increased in both groups from the discontinuation of anesthetic drugs to 10 minutes in PACU compared to before induction. Additionally, compared to the control group, the propofol group showed a slightly high MAP from the discontinuation of anesthetic drugs to 10 minutes in PACU, but no significant difference was found between the two groups. Additionally, the change in HR was not significantly different between the two groups. These results are considered to be because only a small dose of propofol was used in this study, and it did not have a significant effect on the change in MAP and HR during emergence.
The limitation of this study is that first, the concentration of sevoflurane was not measured at the end of surgery, so the effect from the difference in concentration of anesthetic drugs during emergence cannot be excluded. In addition, low-dose remifentanil during emergence has been reported to effectively suppress coughing [11], so although it was discontinued after the end of surgery, it cannot be concluded that the residual effect of remifentanil had no effect on the incidence and severity of coughing in both groups. Although the concentration of sevoflurane was not measured during emergence in this study, the depth of anesthesia was controlled during the anesthesia maintenance by monitoring vital signs and BIS values, and the concentration of sevoflurane and dosage of remifentanil was equal in both groups from 5 minutes before to the end of surgery. Through this, variables that could cause differences in the emergence time were minimized. In addition, more helpful results regarding the effect on coughing during emergence could have been obtained if the study was conducted with an additional group where remifentanil was continued. It is a limitation that this was overlooked, and further study is considered to be necessary regarding this area.
Another limitation of our study is that it was limited to patients receiving nasal surgery, and hence, it cannot predict the coughing suppression effect of propofol during emergence in patients receiving different surgeries. The factors that affect emergence can be diverse according to the type of surgery. Therefore, the study range should be expanded to examine the effect of administering propofol during emergence in patients receiving various types of surgery.
In conclusion, a single dose of propofol 0.3 mg/kg administered at 3 minutes after discontinuing anesthetic drugs significantly reduced the incidence and severity of coughing during emergence in patients who received nasal surgery when anesthetized with sevoflurane and remifentanil.
 XML Download
XML Download