

 PDF
PDF Citation
Citation Print
Print


Introduction
Palonosetron is a 5-hydroxytryptamine-3 (5-HT3) receptor antagonist with a powerful antiemetic effect useful for postoperative nausea and vomiting (PONV) prophylaxis. This agent has great potency and a longer duration of action than other 5-HT3 receptor antagonists including ondansetron, granisetron, tropisetron, and dolasetron [1,2]. PONV is the most common side effect after general anesthesia, occurring in 30-70% of patients according to PONV risk factors [3]. Perioperative use of a 5-HT3 receptor antagonist is highly encouraged to prevent PONV in high-risk patients [4]. Several clinical studies have shown that palonosetron significantly reduces the incidence of PONV [5-8]. However, the safety of palonosetron during the perioperative period has not been established.
5-HT3 receptor antagonists including ondansetron increase the corrected QT (QTc) interval in patients who undergo general anesthesia [9]. Adverse cardiovascular events such as ventricular arrhythmia, myocardial ischemia, and cardiac arrest are also reported after administration of ondansetron [10,11]. Because of a similar pharmacologic mechanism, palonosetron may prolong the QTc interval and increase the risk for critical arrhythmias during general anesthesia. However, perioperative data on the cardiac safety of palonosetron are lacking. Although previous randomized studies reported that palonosetron did not increase the QTc interval in patients undergoing surgery, the primary outcomes of those studies were limited to PONV, and the anesthetic agents that potentially influenced QTc were not identified [7,8]. Because sevoflurane has been associated with QTc prolongation [12], the cardiac effect of palonosetron during sevoflurane anesthesia needs to be evaluated.
We hypothesized that palonosetron would increase the incidence of QTc prolongation in patients under general anesthesia with sevoflurane. This retrospective study was performed to evaluate whether palonosetron can be used safely during general anesthesia with sevoflurane.
Materials and Methods
This retrospective study was performed after approval by the Institutional Review Board of our hospital. The computerized hospital database was reviewed to identify subjects and collect data. We reviewed patients aged 20-90 years who underwent elective laparotomy under general anesthesia with sevoflurane between January and February 2012. We assessed whether palonosetron was administered intravenously during the perioperative period in each patient. Patients who received palonosetron immediately before induction of general anesthesia were enrolled in the palonosetron group. Patients who did not receive any kind of 5-HT3 receptor antagonist intraoperatively were enrolled in the control group. Patients with ischemic heart disease, previous myocardial infarction, congestive heart failure, congenital long QT syndrome, preoperative QTc prolongation > 500 ms, or significant arrhythmias including atrial fibrillation, bundle branch block, or atrioventricular block were excluded, because these are known risk factors for QTc prolongation and torsade de pointes [13]. Patients with an anesthetic duration < 2 h were also excluded.
Routine monitoring of blood pressure, three-lead electrocardiography, oxygen saturation, and body temperature were applied in all patients. Anesthesia was induced with 1.5-2.0 mg/kg propofol, and tracheal intubation was performed after administration of 0.6-0.8 mg/kg rocuronium. Anesthesia was maintained using 1-4 vol% sevoflurane in O2 and air.
Demographic and preoperative data were collected, including age, gender, body weight, height, medical history, preoperative potassium and calcium levels, and electrocardiogram (ECG). All preoperative medications such as antiarrhythmics, antibiotics, and antipsychotics were identified to determine whether they prolonged QTc [14-16]. The lead II ECG data recorded during the operation were retrieved from the server storage system, and ECG data before anesthetic induction, at skin incision, and 30, 60, 90, and 120 min after the incision were obtained. The QT and RR intervals on the ECG trace were measured manually by averaging five successive cardiac beats with a ruler by an anesthesiologist blinded to the patient groups as described previously [9]. The QT interval was defined as the onset of the QRS complex to the end of the T wave, which is the cross point between the descending slope of the T wave and the T-P isoelectric line. To preclude interference of heart rate on the QT interval, the QTc interval was calculated using Fridericia's formula: QTc = QT/RR1/3 [17]. Patients with QTc intervals > 500 ms were identified at 30, 60, 90, and 120 min after skin incision [13]. Changes in the QTc interval from baseline were calculated. Mean arterial pressure, heart rate, body temperature, and expiratory sevoflurane concentrations were also collected at 30, 60, 90, and 120 min after skin incision. Medications administered during general anesthesia such as ephedrine and fentanyl were recorded. The occurrence of arrhythmias during the perioperative period was evaluated.
The statistical analysis was performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). Student's t-test was used to compare continuous variables between the two groups. The chisquare test or Fisher's exact test was used to compare categorical variables. Changes in the QTc intervals measured on the ECG at several time points were analyzed using repeated-measures analysis of variance. Data are expressed as mean ± standard deviation or number of patients (%). P values < 0.05 were considered significant.
Results
We reviewed the electronic medical records of 201 patients who underwent elective laparotomy under general anesthesia with sevoflurane between January and February 2012. Of the 201 patients, 120 were excluded because they did not meet the inclusion criteria. Ultimately, 81 patients were enrolled and analyzed. Of the enrolled patients, 40 who received 0.075 mg intravenous palonosetron (Aloxi®, Helsinn Healthcare, SA, Lugano, Switzerland) immediately before induction of general anesthesia according to the anesthesiologist's preference were assigned to the palonosetron group, and 41 patients who did not receive any kind of 5-HT3 receptor antagonist including palonosetron until completion of surgery were assigned to the control group.
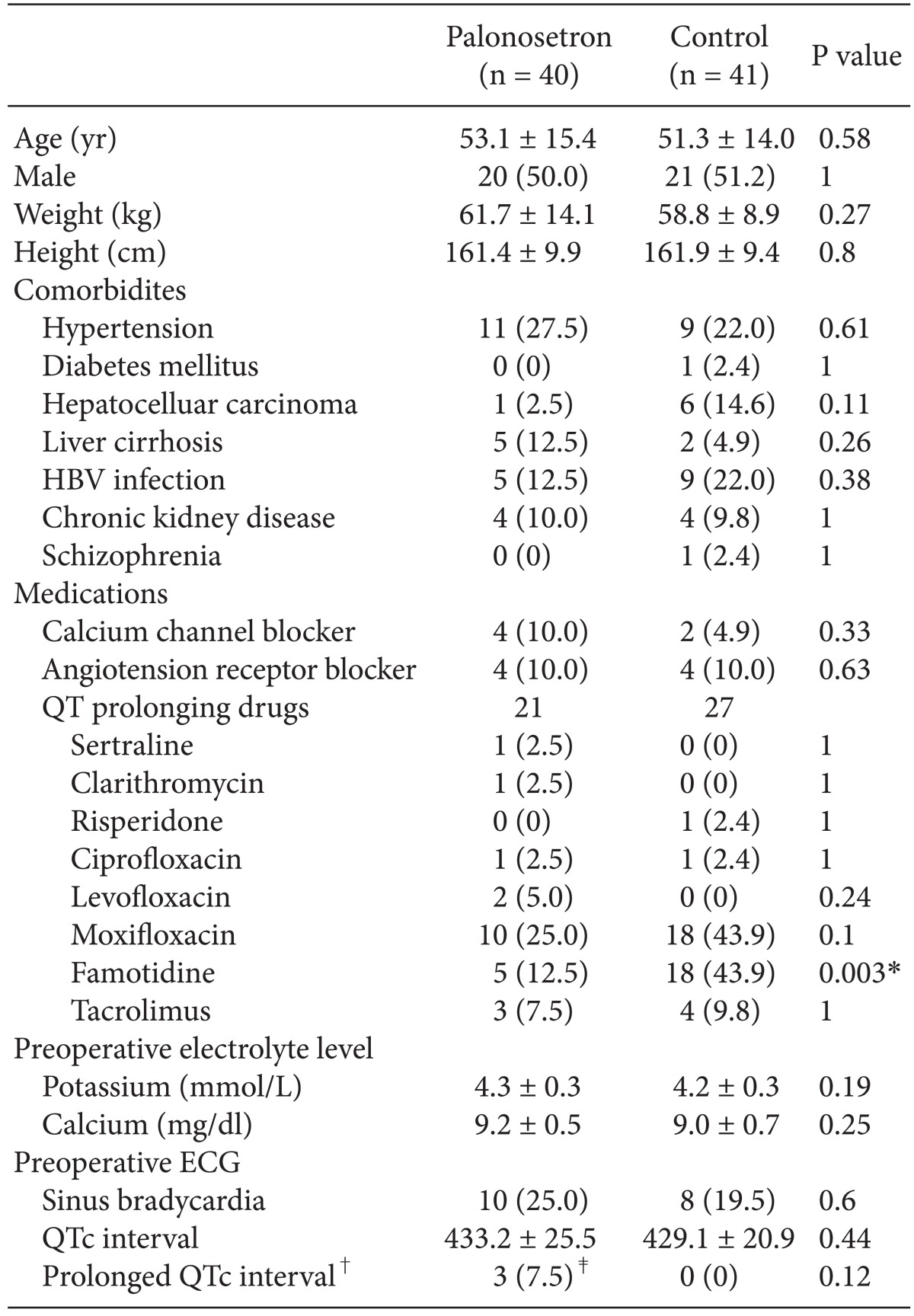
Demographic and preoperative characteristics of the patients are shown in Table 1. Age, gender, coexisting diseases, and medications except famotidine were similar between the two groups (Table 1). Sertraline, clarithromycin, risperidone, ciprofloxacin, levofloxacin, moxifloxacin, famotidine, and tacrolimus, which are QT-prolonging drugs [16], were identified. The number of patients who received at least one of these drugs was not different between the two groups. Preoperative calcium and potassium levels, sinus bradycardia, QTc interval, and the number of patients with a prolonged QTc interval on the preoperative ECG were not different between the two groups (Table 1). The preoperative QTc interval was considered prolonged when it was > 450 ms in male patients and > 470 ms in female patients. None of the patients were hypokalemic before surgery.
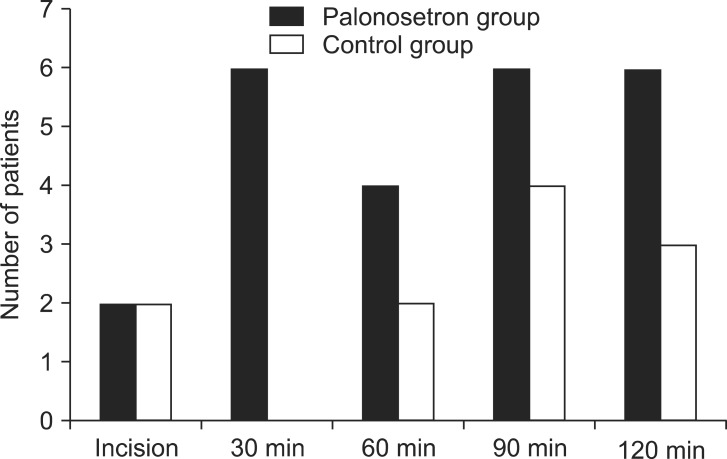
The QTc intervals on the ECG before and during general anesthesia are presented in Table 2. No significant difference in baseline QTc interval was observed between the two groups. The QTc intervals at skin incision and 30, 60, 90, 120 min after skin incision during general anesthesia increased significantly compared to those at baseline in both groups (P < 0.001). The changes in the QTc intervals were not different between the two groups (P = 0.41). The mean individual maximum QTc interval from baseline to 120 min after skin incision was 468.2 ± 33.2 ms in the control group and 471.2 ± 38.0 ms in the palonosetron group (P = 0.70). Fig. 1 shows the number of patients in whom QTc intervals were > 500 ms at each time point during general anesthesia. Six patients in the palonosetron group had a QTc interval > 500 ms 30 min after skin incision, whereas no patient did in the control group (Fig. 1, Table 3). No significant differences were observed between the groups for the number of patients who experienced a QTc interval > 500 ms at other time points except 30 min after skin incision. The proportion of patients who experienced an increase in QTc interval of > 30 or 60 ms was not significantly different between the two groups.
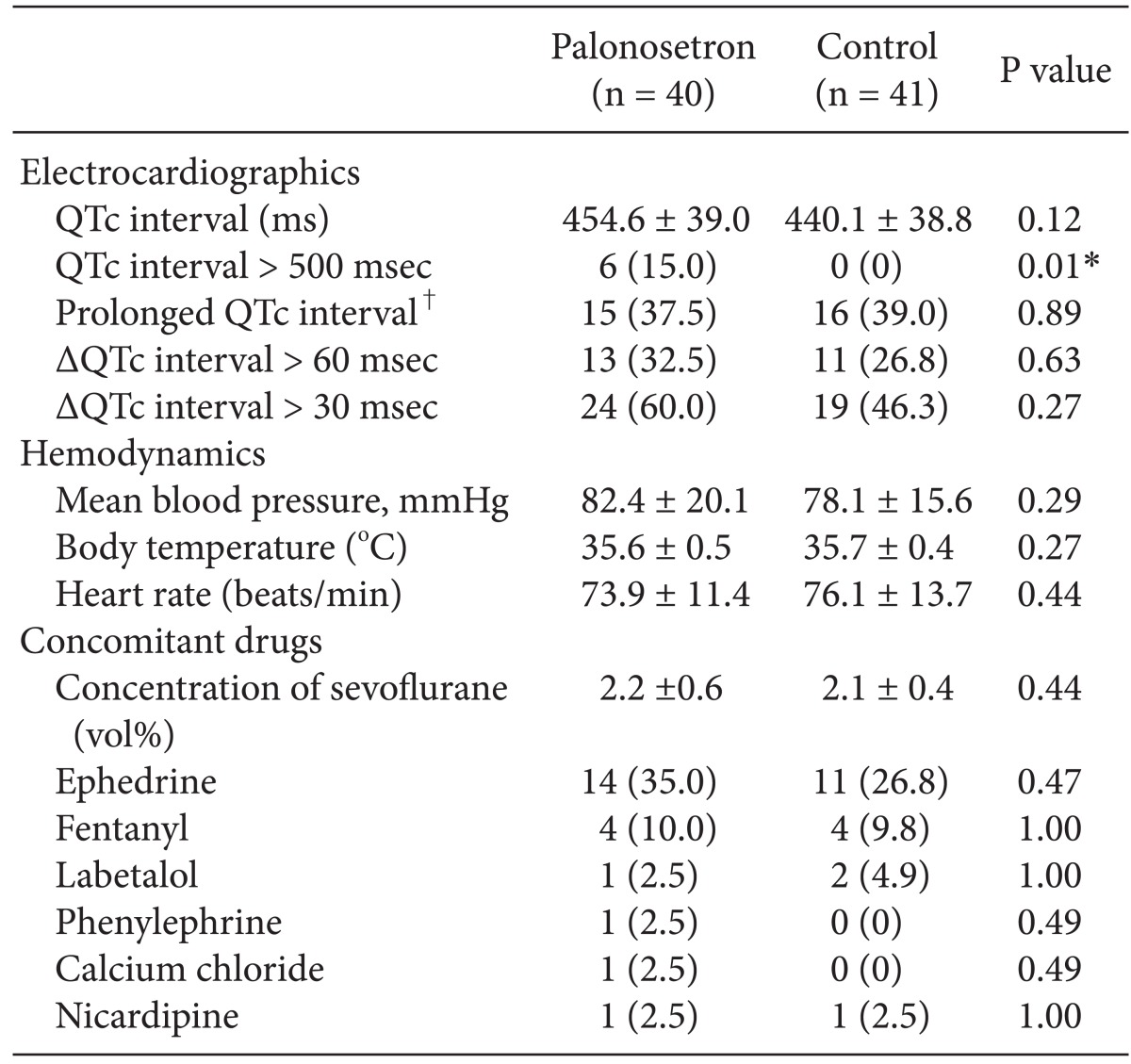
The QTc intervals, hemodynamic values, and medications at 30 min after skin incision are shown in Table 3. No significant differences were observed between the groups for mean blood pressure, body temperature, heart rate, sevoflurane concentrations, and number of patients in whom ephedrine or fentanyl was administered intravenously during anesthesia. A significant arrhythmia occurred in one patient in the palonosetron group. That patient developed ventricular tachycardia at 55 min after skin incision, but his ECG normalized after defibrillation. He presented a higher QTc interval of 521.5 ms at 30 min after skin incision compared to the baseline value of 462.5 ms.
Discussion
The main finding of our study was that the incidence of QTc prolongation > 500 ms increased when patients received intravenous palonosetron before induction of general anesthesia. This QTc prolongation was observed during the initial period of general anesthesia with sevoflurane.
Palonosetron is the safest antiemetic among 5-HT3 receptor antagonists with regard to cardiovascular side effects [1]. The QT interval does not increase significantly after administration of palonosetron in patients with cancer undergoing chemotherapy [18,19]. In some previous prospective randomized dose-ranging studies that targeted patients undergoing surgery, the increase in QT interval was similar regardless of palonosetron administration [7,8]. However, patients with preoperative QTc intervals > 500 ms may have been included in those studies because the preoperative ECG was not confirmed and QT-prolonging risk factors such as hypokalemia, hypothermia, and medications were not identified. In addition, the acute cardiac effects of palonosetron during general anesthesia may have been undetected because the QTc interval measurements were only assessed at 15 min and 3-6 h after palonosetron injection. Moreover, no information was provided about the surgery time interval or QTc measurements. Therefore, the necessity to investigate the relationship between QTc prolongation and palonosetron remains and a clinical study of which the primary outcome is cardiac side effects of palonosetron during general anesthesia is warranted.
Ondansetron, which is another 5-HT3 antagonist, has been associated with QTc prolongation, myocardial ischemia, and fatal arrhythmias in patients undergoing cancer chemotherapy [10] or surgery [9,20]. The exact pharmacologic mechanism has not been established; however, the blocking of cardiac sodium or potassium channels, delays in cardiac repolarization, or coronary vasoconstriction via cardiac 5-HT-receptor have been postulated to precipitate QTc prolongation and significant arrhythmias [21]. Therefore, palonosetron could theoretically have a QTc prolonging effect with a similar mechanism as ondansetron.
In contrast to previous studies [7,8], we found that a QTc interval > 500 ms occurred more frequently after administering palonosetron compared to the control group, suggesting that the combination of palonosetron, sevoflurane, and sympathetic stimulation such as a skin incision may have initiated the significant QT prolongation and ventricular arrhythmia. Similarly, a previous study demonstrated that the additive QT-prolonging effect of isoflurane and anthracycline was due to an increase in the incidence of QTc prolongation in patients undergoing breast surgery [22]. Sevoflurane increases the QT interval in a dose-dependent manner [12,23]. In addition, sympathetic activation, caused by tracheal intubation, surgical incision, or emergence, increases the QT interval [14,24], and this QT-prolonging effect of sympathetic stimulation is prevented by administering an opioid [25,26]. Moreover, we used time points based on the skin incision, which was 35.1 ± 9.9 min after the palonosetron injection, so a surgical stimulatory effect on the QTc interval in addition to the palonosetron effect could have been observed. In the present study, palonosetron may have increased the incidence of QTc prolongation through a combined effect of sevoflurane and surgical stimulation. This is the reason why an increase in QTc interval was not reported in patients with cancer who did not have general anesthesia [18,19]. Our results show that other possible QT prolongation risk factors [18,27-29], including older age, female gender, known QT-prolonging drugs, preoperative QT interval, preoperative bradycardia, preoperative hypokalemia, heart failure, myocardial ischemia, sevoflurane concentrations, temperature, ephedrine, and fentanyl were not different between the two groups.
We observed the ECG during the initial 2 h after injecting palonosetron according to the guidelines [15], which suggest monitoring the QT interval during the peak plasma concentration of the QT-prolonging medication. In a previous report, the time to reach the maximum plasma concentration after intravenous administration of palonosetron was 2-9 min when a dose of 1-3 µg/kg was used in surgical patients [1]. Therefore, a clinical study that investigates the effect of palonosetron during a short period with small intervals after injecting palonosetron is needed. Furthermore, we used Fridericia's formula to calculate the QTc interval, which has less dependency on heart rate compared to that of Bazett's formula [17,26]. Fridericia's formula diagnoses a prolonged QTc interval more correctly because heart rate is very changeable during anesthesia.
This study has several limitations. First, it was not a randomized prospective study. Thus, several factors that may have affected the QTc interval (e.g., a circadian effect, drugs used, and the depth of anesthesia at the time points) were not controlled. However, several risk factors that can affect QT prolongation [14] were similar between the two groups, except famotidine, and we used Fridericia's formula to minimize the effect of circadian heart rate variability in the QTc analysis. Anesthetic management was standardized to maintain a bispectral index of 40-60 in all patients during the study period. Further prospective randomized studies focusing on the cardiovascular effects of palonosetron during general anesthesia are needed. Second, an arrhythmia was detected in only one patient in the palonosetron group, although the incidence of QTc prolongation > 500 ms increased significantly in the palonosetron group 30 min after skin incision. There is controversy about the value of QTc interval, which is considered a surrogate marker for the risk of arrhythmias [30]. However, the QTc interval still remains the standard for monitoring cardiac safety of 5-HT3 receptor antagonists [13].
In conclusion, the incidence of QTc prolongation > 500 ms was higher in patients who received 0.075 mg intravenously administered palonosetron, compared to those who did not during general anesthesia with sevoflurane. Palonosetron may induce QTc prolongation during earlier periods of general anesthesia with sevoflurane.

 XML Download
XML Download