

 PDF
PDF Citation
Citation Print
Print


Introduction
Several studies have shown that volatile anesthetics do not suppress hemodynamic reactions [1] and the release of catecholamines [2] induced by noxious stimulation. In animal experiments, volatile anesthetics suppress somatic responses by anesthetic effects within the spinal cord and not within the brain [3]. This suggests that, during general anesthesia, volatile anesthetics may have only sedative and not analgesic effects.
In addition, with an increase in the performance of ambulatory surgery, early recovery from anesthesia is required, while intraoperative awareness must be avoided by administering a sufficient concentration of volatile anesthetics. However, the requisite anesthetic concentration of sevoflurane required to obtain sufficient sedation level with adequate analgesia and muscle relaxants has not been determined in a clinical setting, despite the fact that insufficient use of analgesics or muscle relaxants may result in awareness during general anesthesia. The purpose of this study was to determine the requisite concentration of sevoflurane required to obtain a suitable anesthesia level during combined epidural-general anesthesia determined by bispectral index monitoring. In addition, as increasing age was found to reduce sevoflurane requirements to suppress responses to a verbal command [4], we investigated the influence of age on the concentration in this study.
Materials and Methods
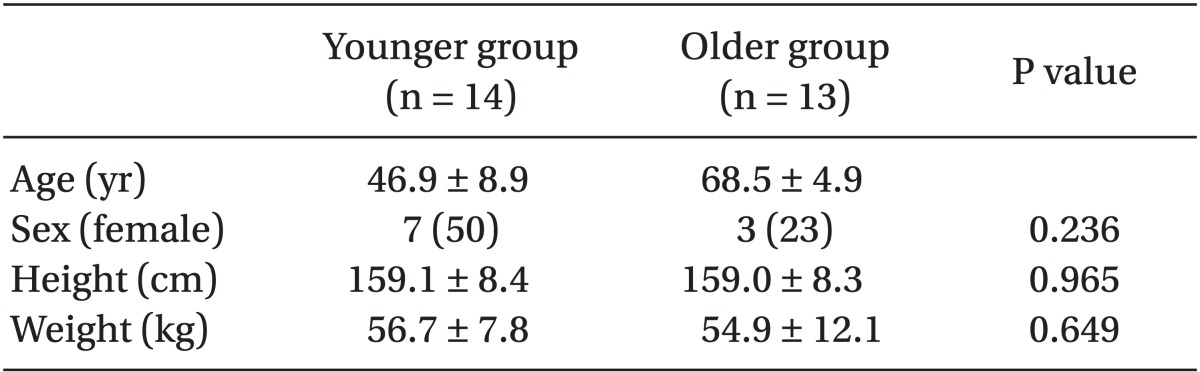
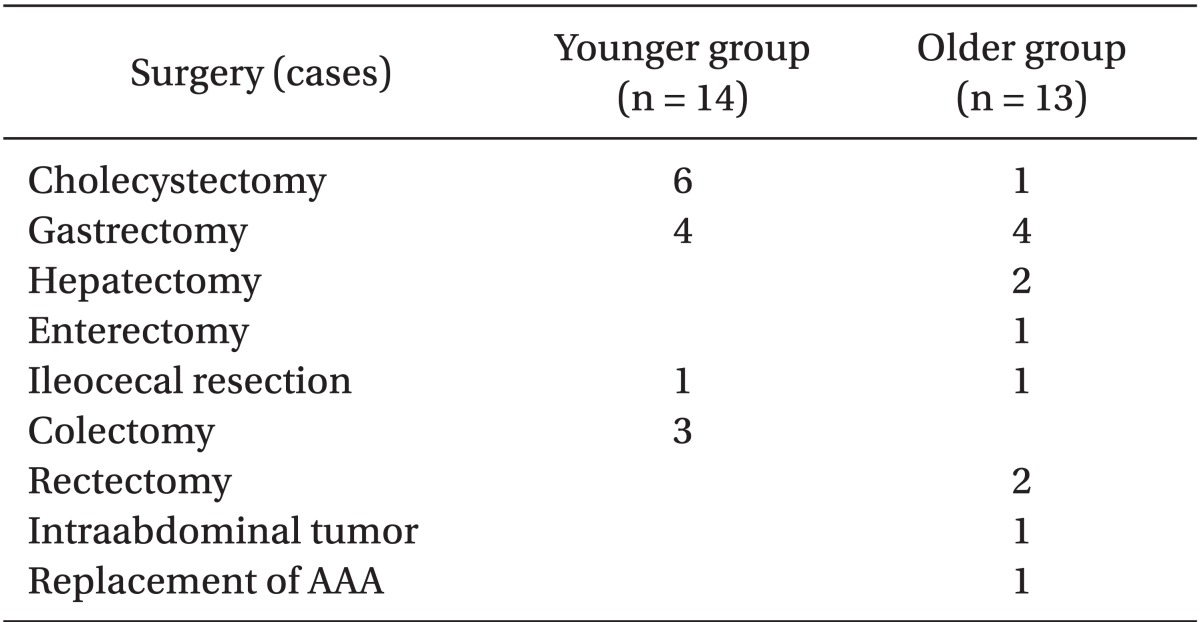
The study protocol was approved by our institutional ethics committee and informed consent was obtained from each patient. Twenty-seven selected patients (American Society of Anesthesiologists physical status I-II) undergoing abdominal surgery were enrolled (Table 1). The patients were divided into two groups: age 30-59 and age 60-75 (Table 1). The type of surgery is described in Table 2. Criteria for exclusion included body weight less than 40 kg or more than 80 kg, cerebrovascular diseases, seizure disorder, developmental delay, and known allergy to any drugs.
Patients received no premedication and were scheduled for combined epidural-general anesthesia. An epidural catheter was inserted via T 10-11 or T 11-12, and after a test dose, 10-20 ml of 1% lidocaine was administered, immediately followed by continuous infusion of 1% lidocaine at a rate of 10 ml/hr. All patients received 2 mg/kg propofol and 0.15 mg/kg vecuronium for tracheal intubation. Anesthesia was maintained with 4 L/min air, 2 L/min oxygen, and sevoflurane. Ventilation was adjusted to maintain arterial carbon dioxide partial pressure at 35-40 mmHg. We excluded patients whose heart rate or systolic blood pressure increased to more than 15% above baseline at the start of skin incision, because of inadequate epidural anesthesia. Neuromuscular blockade was measured by acceleromyography, with the TOF-Watch (NV Organon, Oss, the Netherlands), and additional vecuronium was given at the appearance of a T2 twitch in a train-of-four ratio. The expired concentrations of anesthetics were monitored using a Capnomac Ultima (Datex, Helsinki, Finland). The bladder temperature was monitored continuously and was maintained at normothermia (36.0-37.0℃) with a water blanket (Medi-Therm II; Gaymer, NY, USA).
Prior to induction of anesthesia, the electrodes for bispectral index (BIS) (BIS Sensor; Aspect Medical Systems, Natick, MA, USA) were applied to the forehead. The BIS was monitored continuously using an Aspect A-1050 monitor (BIS version 3.4; Aspect Medical Systems, MA, USA). Initially, the patient was given 1.0 vol% end-tidal sevoflurane, and the BIS value was monitored. If the patient had an average BIS of greater than 60, the sevoflurane concentration was increased in a stepwise fashion; whereas if the patient had a BIS of less than 40, the sevoflurane concentration was decreased also in a stepwise fashion until BIS values remained between 40 and 60. The concentrations of sevoflurane utilized were 0, 0.2, 0.6, 0.8, 1.0, 1.5, 2.0, 2.5, and 3.0 vol%. During surgery, inspiratory and end-tidal concentrations of sevoflurane and BIS values were recorded every 5 minutes. In all patients, gradual reduction of sevoflurane concentration was started when the surgeons began the closure of the peritoneum, and was discontinued at the end of surgery. Time to extubation after surgery was recorded.
All patients were assessed for awareness of surgery the day after operation. After confirming that the patients could recall events before the surgery and events after it, they were asked if they could recall any events during the operation. This approach may reduce false-negative results of awareness during surgery.
Statistical analysis
Statistical analyses were performed with the computerized program Statistical Package for the Social Sciences (SPSS 19.0, Chicago, IL, USA). Data are presented as the mean ± standard deviation [minimum-maximum]. Categorical variables are described using number (%); and they were compared using chi square test or Fisher's exact test. All P values are two-tailed. P values less than 0.01 were considered significant.
Results
Preoperative profiles of the patients are summarized in Table 1. Neither height nor weight differed between the groups, although in the older group, male (n = 10) outnumbered female (n = 3).
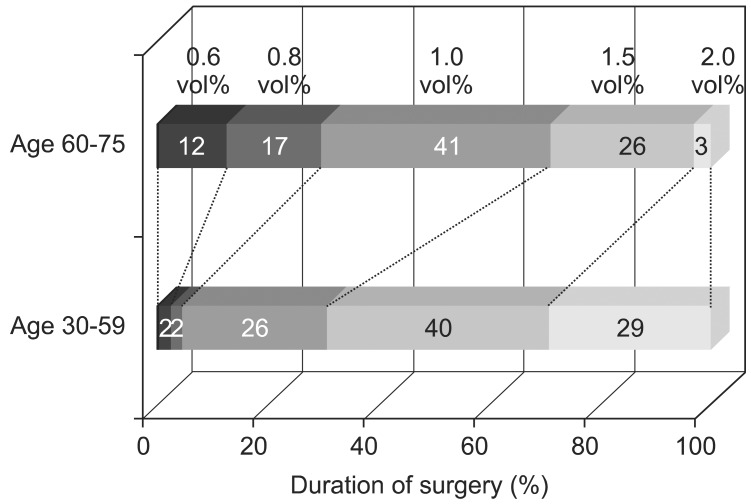
Time course during surgery is shown in Fig. 1. The duration of surgery was significantly longer in the older group (268.1 ± 71.4 [170, 450] minutes) than in the younger group (171.1 ± 78.1 [50, 285] minutes) (P < 0.01). In the younger group, the maximum concentration of sevoflurane needed during surgery was 1.95 ± 0.14 (95% confidence interval: 1.87-2.10) vol%, while it was 1.54 ± 0.44 (95% confidence interval: 1.27-1.80) vol% in the older group (P < 0.01). There were no differences in the interval of assessment from the end of surgery to extubation between the two groups (P = 0.916). However, the requisite sevoflurane concentration required to maintain a BIS of 40-60 was not stable during the surgery in either group (Fig. 1). In the younger group, it was 1.0 vol% over 26% of the total duration of surgery, 1.5 vol% over 40% of surgery, 2.0 vol% over 29% of surgery, and 2.5 vol% over less than 1% of surgery. In the older group, it was 0.8 vol% over 17% of surgery, 1.0 vol% over 41% of surgery, and 1.5 vol% over 26% of surgery. In addition, 2.0 vol% was needed over only 3% of surgery as end-tidal concentrations of sevoflurane.
Postoperative interviews revealed no awareness during surgery.
Discussion
Our study demonstrated that the requisite sevoflurane concentration for adequate sedation with combined epidural-general anesthesia was, as end-tidal concentration of sevoflurane, 2.5 vol% for the younger group and 2.0 vol% for the older group as determined by BIS monitoring. In addition, we reviewed all anesthesia records and did not find any signs of inadequate analgesia such as sudden increase in blood pressure and/or heart rate when the sevoflurane concentration was increased according to the BIS value. We believe that these percentages are sufficient to avoid awareness during surgery if adequate analgesia has been supplied.
If sufficient analgesia were obtained, we would expect that the requisite sevoflurane concentration for sufficient sedation determined by BIS monitor would be variable to some extent, because the strengths of noxious stimuli change with various surgical procedures. In this study, this parameter did exhibit some fluctuations. This also indicates that with weak stimuli, the maximum concentration of sevoflurane (2.5 vol% for the younger group and 2.0 vol% for the older group) does not need to be administered to obtain sufficient anesthesia. In some patients, BIS monitor did not change with blood pressure and heart rate increase during surgery, indicating no need for increase of sevoflurane concentration. Our anesthesia records did not include detailed notes on the surgical stimuli, and we could not elucidate the reasons for these phenomena in detail. Further studies are warranted.
Compared with other studies, the requisite sevoflurane concentration of this study was somewhat higher than we expected. Hodgson and Liu [5] found that 0.73 vol% sevoflurane was required in epidural-general anesthesia with no stimuli, and that epidural anesthesia reduced the amount of sevoflurane required. Unfortunately, this small percentage could not rule out the possibility of the premedication with midazolam and fentanyl having an effect. However, Olofsen and Dahan [6] demonstrated that the sevoflurane concentration at which 50% depression of electroencephalogram parameters occurred was 1.14 ± 0.31 vol%. In addition, Katoh et al. [7] reported that the ED50 of sevoflurane for skin incision was 1.92 vol%. These percentages appear compatible to our own.
It may seem excessive to administer 2.5 vol% of sevoflurane in the younger group and 2.0 vol% in the older group, as most of the patients did not recall anything under 2 vol% of sevoflurane for the younger group and 1.5 vol% sevoflurane for the older group. In this study, to avoid an anesthesia level of a BIS of more than 60, we maintained 2.5 vol% of sevoflurane for a very short time in only one person. Actually, the duration of this application of 2.5 vol% was only 20 minutes in a total of 300 minutes in this patient with total gastrectomy. In addition, in this patient, 1.5 vol% sevoflurane for 155 minutes and 2.0 vol% for 105 minutes were administered. To avoid BIS of more than 6o, we maintained 2.5% sevoflurane. Avoiding a BIS of more than 60 did not mean avoiding recall during surgery. In a very short time, we may not have to maintain BIS precisely at less than 60 to avoid memory recall during surgery. We calculated that the 95% confidence interval of maximum concentration of sevoflurane to be 1.87-2.10 vol% in the younger group and 1.27-1.80 vol% in the older group. The concentration of 2.5 vol% for the younger group and 2.0% for the older group may seem high in clinical settings. It is clearly shown that no more than 2.5 vol% in the younger group and 2.0 vol% in the older group needs to be administered for adequate analgesia.
We avoided administering premedication, because of the synergistic effect on the patient's sedative state. In addition, we avoided the use of nitrous oxide as it causes dramatic changes in the raw electroencephalogram (EEG) [8] due to different sites of effect: the N-methyl-d-aspartate (NMDA) receptor for nitrous oxide [9]; and the gamma-aminobutyric acid (GABA) type A receptor for sevoflurane [10]. In addition, to avoid the effects of electromyography (EMG) [11] and body temperature [12], acceleromyography was used, and the body temperature was maintained at a constant level.
Concerning the limitation of monitoring, we used an Aspect A-1050 monitor (BIS version 3.4), which did not avoid the effects of electrocautery and electromyogram efficiently. Such may be one of the reasons for the variation in the minimal required sevoflurane concentration observed. The newer version, BIS-XP (BIS version 4.0), has a novel algorithm [13,14] and enhanced removal of effects.
Our study had several other limitations. The number of patients was small, and the surgeries that the patients underwent were variable, implying varying strengths of noxious stimuli. In future studies, by selecting patients undergoing a certain type of surgery and using a newer monitoring system, we may be able to obtain more precise data concerning the minimum sevoflurane concentration required for sedation during surgery.
In conclusion, the requisite concentration of sevoflurane with combined epidural-general anesthesia was 2.5 vol% for the younger group and 2.0 vol% for the older group, as determined by BIS monitoring. We believe that these ratios are sufficient to avoid awareness during surgery with adequate analgesia.
 XML Download
XML Download