

 PDF
PDF Citation
Citation Print
Print


Introduction
Supraclavicular block provides excellent anesthesia for upper limb surgery [1,2]. Moreover, ultrasound guidance in supraclavicular block has been introduced and gaining popularity [3]. Ultrasound-guided supraclavicular block has many advantages including the higher success rate, faster onset time, and fewer complications [4-6]. In the previous studies on the ultrasound-guided axillary blocks and interscalene blocks, the possibility of the reduced volume of local anesthetics was demonstrated [7-10]. However, there is some controversy in such reduced anesthetics volume in the ultrasound-guided supraclavicular block [11,12].
In the previous studies on the minimum effective volume for the ultrasound-guided supraclavicular block, the Dixon and Massey up and down method (DUDM) and biased coin design up and down method (BUDM) were used to calculate the minimum effective volume (MEV) 50, MEV90, and MEV95, respectively [11,12]. These effective volumes were speculated by statistical calculation. However, Orebaugh et al. [13] indicated that the results from the DUDM may be different from those of the clinical practice, and the comparison of the varied anesthetic volumes in the clinical practice has not been studied in the ultrasound-guided supraclavicular block.
The aim of this study was to examine the clinical data according to the varied volumes of local anesthetics in the ultrasound-guided supraclavicular block.
Materials and Methods
After the approval of Institutional Review Board and obtaining patients' written informed consent, one hundred twenty patients undergoing forearm and hand surgery were randomly assigned to one of four groups to receive ultrasound-guided supraclavicular block with 1% mepivacaine 35 ml (Group 35), 30 ml (Group 30), 25 ml (Group 25), or 20 ml (Group 20). Exclusion criteria included patients with diseases affecting sensory or motor functions of the upper extremity, pregnant patients, allergy to local anesthetics, and contraindication to regional anesthesia.
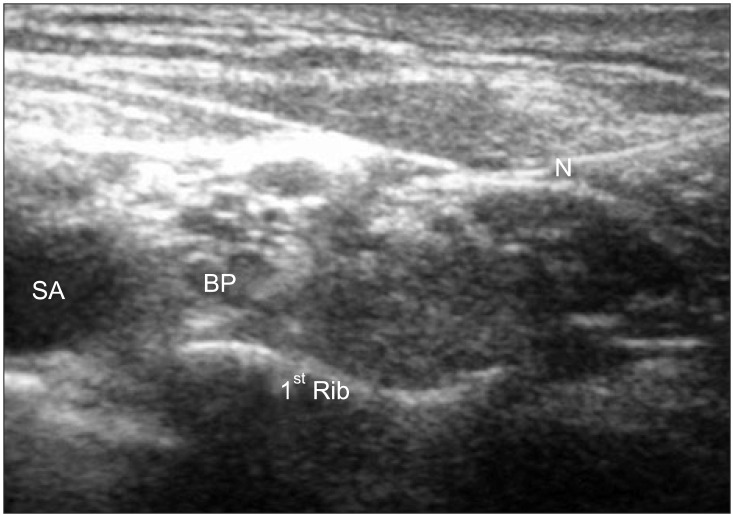
For ultrasound-guided supraclavicular block, an ultrasound machine (Vivid I®, GE Yokogawa Medical Systems Ltd., Tokyo, Japan) and a 12 MHz linear type probe were used. The supraclavicular fossa was scanned to locate the subclavian artery and brachial plexus cluster after skin preparation. After local infiltration of skin, a 22 gauge, 5 cm, short beveled insulated needle (Stimuplex® A, B. Braun, Melsungen AG, Germany) was advanced from the lateral to medial in the long axis of the ultrasound beam. Once the needle tip was located around the brachial plexus cluster (Fig. 1), a nerve stimulator (Stimulpex®, B. Braun, Melsungen AG, Germany) was turned on with 2 Hz, starting from 1.0 mA down to 0.5 mA. Local anesthetic was injected in real time with the presence of muscle twitch with the nerve stimulation. If no motor response was obtained, the injection was performed under ultrasound imaging alone without nerve stimulation. In order to avoid intraneural injection, we confirmed that the location of the needle tip was not in the nerves before each injection. However, the needle tip was not always visualized. Therefore, 0.5 ml of 1.5% mepivacaine was injected as a test dose. If patients did not complain of paresthesia or pain, or the injection pressure was not high, the remaining dose of 1.5% mepivacaine was injected incrementally with withdrawing the needle. If local anesthetic did not reach some parts of the brachial plexus, the needle was repositioned until the appropriate image was obtained.
We checked the sensory anesthesia with 26 gauge needle every 5 minutes up to 30 minutes after injection of local anesthetic in all 5 cutaneous nerve distributions (musculocutaneous nerve: lateral side of the forearm, radial nerve: dorsum of the hand over the 2nd metacarpophalangeal joint, ulnar nerve: little finger, median nerve: medial thenar eminence, and medial cutaneous nerve: medial side of the forearm) by a research assistant who was blinded for over 30 minutes after the injection of local anesthetic. The onset of anesthesia was defined as a complete sensory anesthesia in each of the nerve distributions.
We analyzed the success rate in two aspects: the success rate of each nerve and all five nerves. The success rate of each nerve was named 'individual nerve's success rate', and the success rate of all five nerves was termed 'complete success rate'. The successful block of individual nerve was defined as the onset of sensory anesthesia in each nerve's distributions, and a complete successful block was defined as a complete sensory anesthesia in all 5 cutaneous nerve distributions of the forearm at 30 minutes after the local anesthetic injection and operability. Then, all patients were checked for complications such as Horner's syndrome, voice changes, and chest discomfort. The patients who had failed blockades had general anesthesia or sedation with midazolam and pethidine.
Statistical analysis was performed with SPSS version 12. The sample size (n = 120) was determined based on the following criteria: a significance level of 5% and a power of 80% from the pilot study. The age, height, weight, and onset time of block were compared among the four groups by one-way analysis of variance (ANOVA) and Tukey post hoc tests. The age, height, weight, and body mass index were also compared between the successful and failed cases. For intergroup comparisons, the distribution of data was first evaluated for normality using the Shapiro-Wilk test. The normally distributed data and non-normally distributed data were compared using Student's and Mann-Whitney test, respectively. The sex, success rate, and the incidence of complications were compared using Chi-square test or Fisher's exact test. A P value < 0.05 was considered significant.
Results
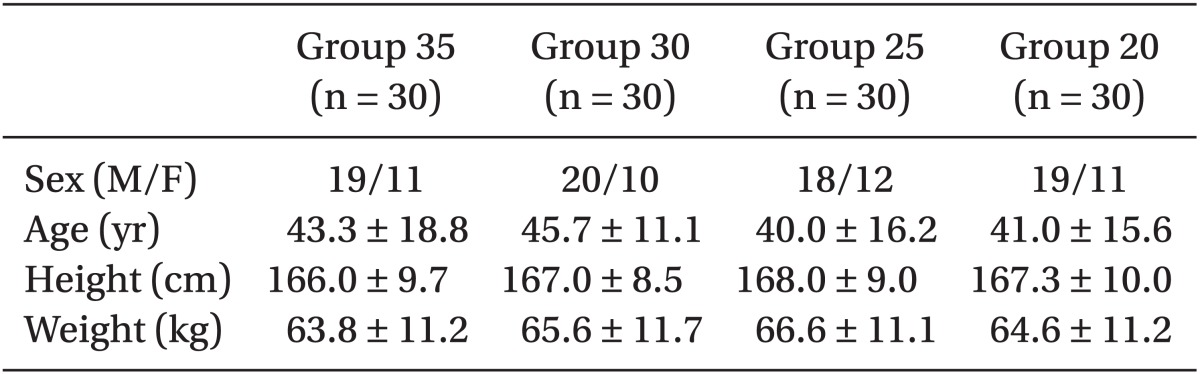
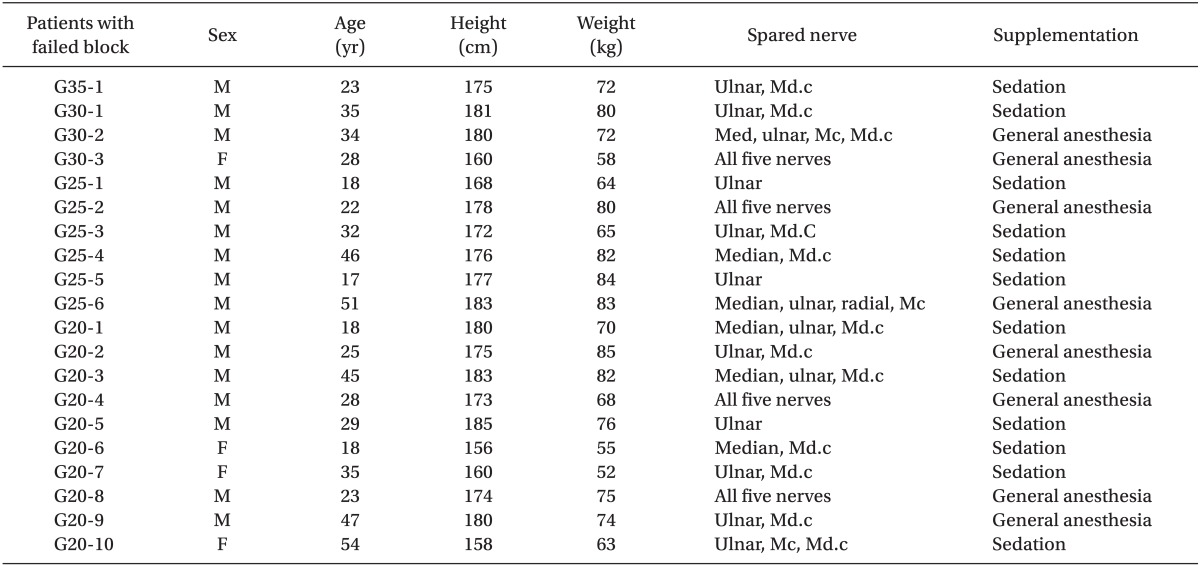
One hundred twenty patients were included in this study. There were no differences in the characteristics between the four groups (Table 1).
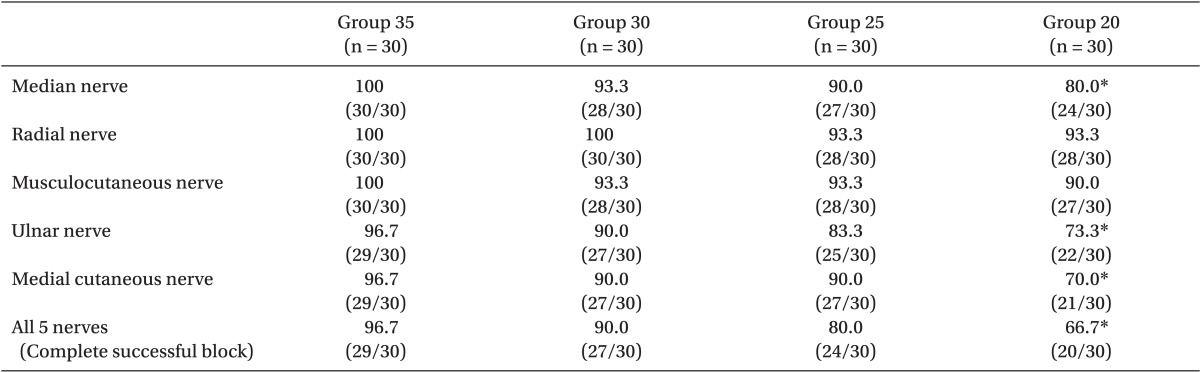
The complete success rates of Group 35, Group 30, Group 25, and Group 20 were 96.7%, 90.0%, 80.0%, and 66.7%, respectively. The success rate of Group 20 was lower than that of Group 35 (P < 0.05) (Table 2). The individual success rate of the ulnar nerve and medial cutaneous nerve were lower than those of other nerves (P < 0.05) (Table 2).
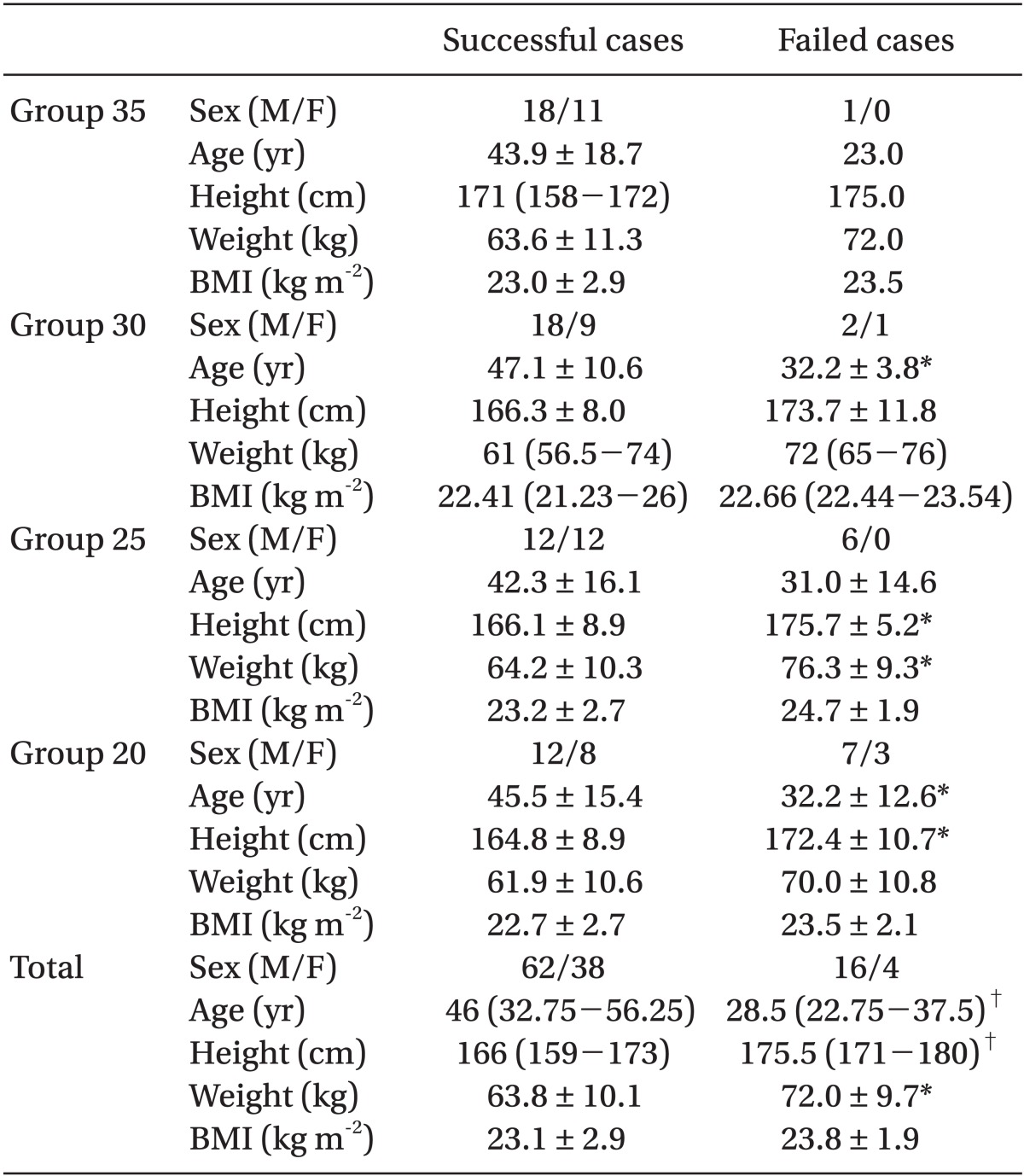
The average height and weight in failed cases were larger than those in the successful cases (P < 0.05) (Table 3). In Group 35, one failure was operated under sedation only. In Group 30, one failure was operated under sedation, and another two failures received general anesthesia. In Group 25, four failures were given sedation only, and 2 failures received general anesthesia. In Group 20, six failures were operated under sedation only, and four failures received general anesthesia (Table 4).
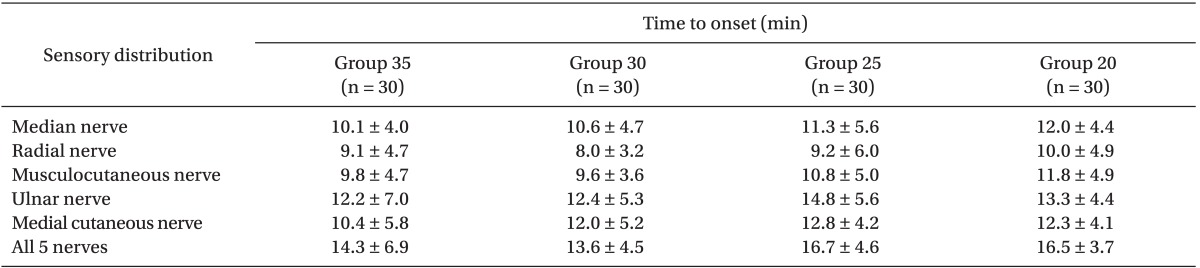
The average onset times of the five nerves were 14.3 ± 6.9 min (Group 35), 13.6 ± 4.5 min (Group 30), 16.7 ± 4.6 min (Group 25), and 16.5 ± 3.7 min (Group 20), respectively. There were no significant differences (Table 5).
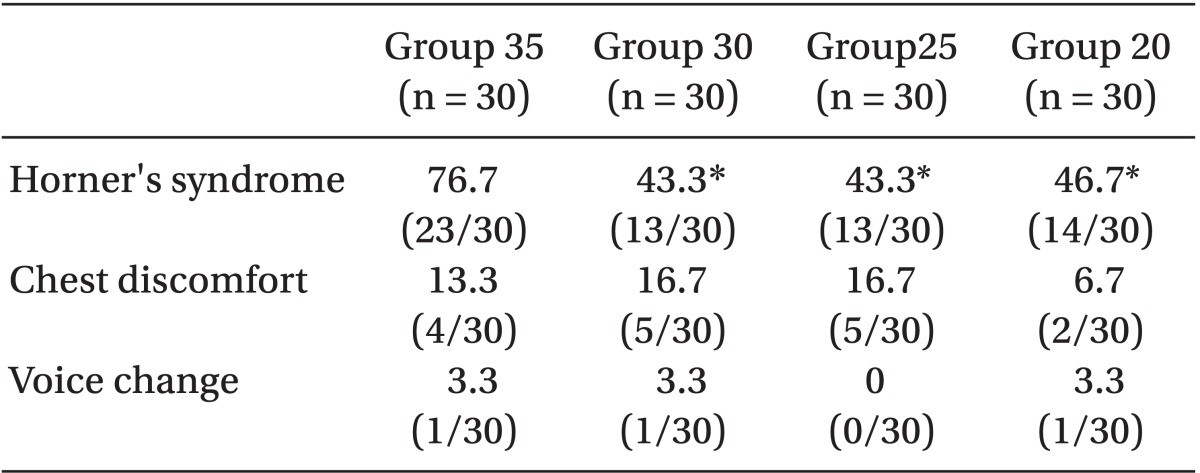
Horner's syndrome in Group 35 was higher than other groups (P < 0.05). There was no significant difference in the incidences of chest discomfort and voice change (Table 6).
Discussion
Systemic local anesthetic toxicity is still frequent and dose dependent. Therefore, reducing the dose of local anesthetic in regional anesthesia can contribute to the safety of regional anesthesia [1]. Some authors demonstrated the possibility of dose reduction in ultrasound-guided axillary blocks and interscalene blocks [7-10]. However, such possibility in ultrasound-guided supraclavicular block is controversial [11,12].
Duggan et al. [11] estimated MEV95 and MEV50 to be 42 ml and 23 ml, respectively, using DUDM. According to the study results, it was concluded that they could not reduce the volume of local anesthetic in ultrasound-guided supraclavicular block. Tran et al. [12] calculated MEV90 to be 32 ml, using BUDM for ultrasound-guided supraclavicular block in their study. This volume (32 ml) for 90% success rate was lower compared with the conventional technique using 40 ml of local anesthetics. However their results were derived from the estimated values using BUDM. The limitations of Duggan et al.'s study were the wide confidence interval and no comparison with the conventional supraclavicular block [11]. The limitations of Tran et al. [11] were that the operators were trainees and 16-point scale including motor block was used for definition of successful block [12]. Therefore, we think that their estimated MEV90 (32 ml) may be larger than the local anesthetic volume for surgical anesthesia.
Orebaugh et al. [13] indicated that the results from DUDM do not seem to be easily translated to the clinical practice of peripheral nerve blockade. Therefore, we decided to perform a clinical comparison of the success rates with varied volumes of local anesthetics in ultrasound-guided supraclavicular block.
Before the commencement of the study, we planned the study with 40 ml, 35 ml, 30 ml, 25 ml and 20 ml of local anesthetic based on the results (MEV 95 = 42 ml, MEV90 = 32 ml, and MEV 50 = 23 ml) from the previous studies [11,12]. However, the success rate of ultrasound-guided supraclavicular block with local anesthetic 35 ml in the preliminary study was 94.7%, which was similar to MEV95 in Duggan et al. [11]. For this reason, we excluded the 40 ml of local anesthetic volume in the study.
In general, the volume of local anesthetic for conventional supraclavicular block is known to be 40 ml [14]. A 90.3% success rate was achieved with the traditional technique using 40 ml local anesthetics [15]. Ultrasound-guided techniques allowed for the reduction of the volume to 30 ml of mepivacaine 1% with an equivalent success rate. Therefore, we could state that the volume of local anesthetics could be reduced. In addition, this volume was similar to MEV90 (32 ml) from Tran et al. [12]. However, this result was disappointing.
We expected to reduce the local anesthetic volume to be 20 ml in ultrasound-guided supraclavicular block before commencing the study, because the minimum effective volume could be reduced to 8-20 ml in the ultrasound-guided axillary blocks [7,8].
We suggest a possible explanation as to why we could not reduce the volume of local anesthetic to be 20 ml as we expected in spite of using ultrasound. Cornish et al. [16,17] injected contrast dye into the tunnel that surrounded brachial plexus and observed various patterns of flow within the tunnel. The dye did not spread homogeneously. With this observation, they asserted that the brachial plexus was surrounded within the rigid-walled tunnel as differently from the simple tubular structure, such as a sheath. In simple tubular structure, the local anesthetic injected at one point can spread throughout the tunnel. However, compartmentalization is present in the rigid tunnel, because the layers of connective tissue are not homogeneous. Therefore, the injection at one point in this rigid-walled tunnel may not spread to other nerves in the tunnel. With this theory, we presumed that the lower volume of local anesthetic was not able to spread to all nerves in this study.
At this point, we wondered why the reduction of local anesthetic in ultrasound-guided axillary block could be possible [7,8]. We assumed that four nerves (radial, median, ulnar, musculocutaneous nerve) could be distinguished by ultrasound, and injected 3-5 ml of local anesthetic to each nerve in the axillary region. However, in the supraclavicular region, each nerve could not be distinguished, it is located in the form of a cluster. Therefore, the local anesthetics should be filled in the tunnel, thus permitting no marked reduction in the volume from that used traditionally.
We also found that the height and weight were larger in the failed cases (P < 0.05) (Table 3). With this finding, we compared the differences under the condition with same local anesthetic volume (Group 35, Group 30, Group 25, and Group 20). As a result, the height and weight of failed cases were larger in Group 25, and the height of failed cases was larger in Group 20. The age in Group 20, Group 30, and the total patients were lower in the failed cases (P < 0.05). Therefore, the rigid-walled tunnels containing the brachial plexus in the supraclavicular region may be larger in the failed cases, but it is difficult to conclude such with the limited data of this study. Thus, we suggest that further studies should be performed to elucidate the factors influencing the success rate.
In our study, the success rates of ulnar and medial cutaneous nerve were lower than those of other nerves. This can be explained by the brachial plexus anatomy and the approach technique used in this study. The ulnar and medial cutaneous nerves are derived from the inferior trunk of brachial plexus. The approach to inferior trunk is difficult by lateral to medial approach in plane used in this study. As the needle advances through the brachial plexus bundle to reach the inferior trunk, there may be a nerve damage. We suggest that different approach techniques (e.g. multiple approach including the out of plane technique) should be applied to increase the success rate with the lower volume of local anesthetics.
There were some patients who complained of chest discomfort in this study. However, the chest X-ray was not taken since pneumothorax was not a concern, and no patients complained of chest discomfort after the surgery. We presume that transient hemi-diaphragmatic paresis may have occurred in some of the patients with the chest discomfort.
In conclusion, we achieved 90% success rate with 30 ml of 1% mepivacaine. This result corresponds to MEV90 in the previous study using BUDM. Therefore, we suggest 30 ml of local anesthetic volume for the ultrasound-guided supraclavicular block.
 XML Download
XML Download