

 PDF
PDF Citation
Citation Print
Print


Introduction
Postoperative liver and kidney function are affected by anesthetics and their metabolites, as well as by sympathetic stimulation, decrease in blood perfusion, underlying diseases, viral hepatitis, sepsis, drug reactions, side effects and damage from surgeries [1,2]. Halothane, which is a typical inhalational anesthetic, is known for its liver and kidney toxicity. A new inhalational anesthetic, sevoflurane, has recently been developed and is now frequently used. Total intravenous anesthesia (TIVA) with propofol is commonly used as an ideal balanced anesthesia. Because TIVA is known to have early emergence from general anesthesia and can reduce postoperative nausea and vomiting, it is becoming favored as a general anesthetic [3]. TIVA with propofol is expected to have a lower risk of direct damage from anesthetic metabolites, and shows hemodynamic stability during anesthesia [4]. However, few prospective studies have been performed on the effects of inhalational anesthetics and TIVA on liver and kidney function. In addition, previous studies comparing sevoflurane and propofol have variable results [5,6] with small sample sizes (20-40), and limited ability to analyze the effects of anesthetics, because they included patients who underwent surgeries that could directly affect liver and renal function.
In the present study, we examined differences in postoperative liver and kidney function when using inhalation anesthesia with sevoflurane or TIVA with propofol. The present study was performed in a sample of patients who underwent thyroidectomy, a surgery that has no direct effect on the liver and kidney.
Materials and Methods
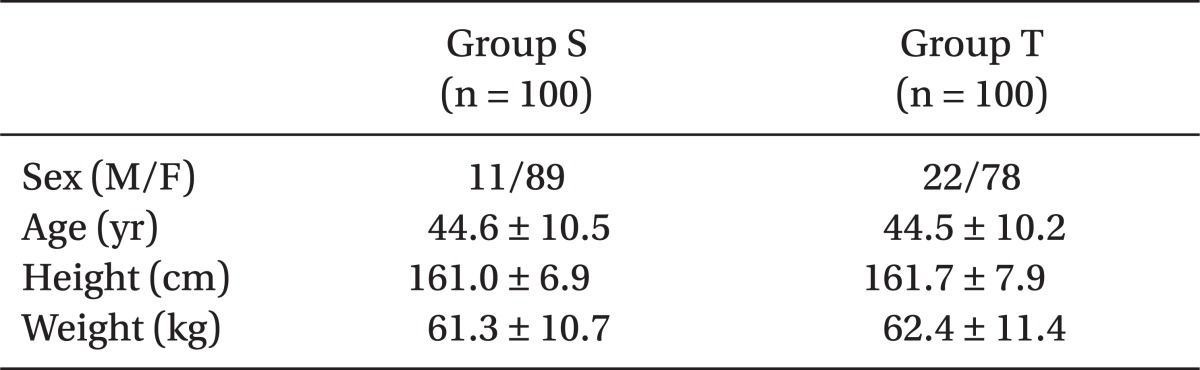
The study was done using a sample of 200 American Society of Anesthesiologists physical status I and II patients who were scheduled for thyroidectomy, between the ages of 20-65 years. The Institutional Review Board approved this study. The purpose and methodology of the study were explained to patients before obtaining consent. Patients with liver or kidney abnormalities, hypertension or diabetes, surgical history in the past month and intraoperative hypotension, or blood transfusion were excluded from the study. The patients were randomly assigned to two groups of 100 patients each. The two groups were Group S, which received sevoflurane and remifentanil, and Group T, which received TIVA with propofol and remifentanil with a target controlled infusion pump (TCI pump). There were no differences in sex, age, height, and weight between the two groups (Table 1).
All patients were premedicated with 0.05 mg/kg midazolam (Dormicum®, Roche, Switzerland) and 50 mg ranitidine (Urantac™, Whanin, Korea) for 30 min before undergoing anesthesia. Venous access was secured with an 18G needle, and lactated Ringer's solution was infused at 2 ml/kg/hr. For anesthesia induction, spontaneous breathing with 100% oxygen was performed for 2 min for denitrogenation. Then, 0.2 mg glycopyrrolate (Mobinul™, Myungmoon, Korea) was administered. To induce loss of consciousness, Group S received 0.05 mg/kg midazolam and 1 mg/kg propofol (Provive™, Claris, India), and remifentanil was administered using an infusion pump at a rate of 10 ug/kg/hr. In Group T, a TCI pump (Ochestra Base Premea, France) was set for propofol at 4 ug/ml and remifentanil (Ultiva™, GSK, Italy) at 4 ng/ml as the effect-site concentration. For tracheal intubation, 0.9 mg/kg rocuronium (Esmeron®, Organon, Netherlands) was administered 90 sec after the patient was intubated. For anesthesia maintenance, controlled ventilation was conducted to maintain the ETCO2 at 30-35 mmHg with O2 : air = 1.5 L/min : 2.5 L/min, the respiratory rate at 10-12 breaths/min, and the tidal volume at 7-10 ml/kg. Group S received 1-2% sevoflurane with continuous infusion of remifentanil (2-15 ug/kg/hr) using an infusion pump. Group T used the TCI pump and the effect-site concentration of propofol and remifentanil was adjusted to SBP ± 20% of baseline. The bispectral index (BIS, Vista™, USA) was maintained at 40-60. For muscle relaxation, vecuronium (Vecron™, Myungmoon, Korea) was used intermittently. For fluid administration during surgery, lactated Ringer's solution was administered at 4-6 ml/kg/hr, depending on urine output and blood loss. Along with BIS, blood pressure, EKG, SpO2, ETCO2, and body temperature were monitored during surgery. To evaluate liver and kidney function, aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urea nitrogen (BUN), and creatinine were checked preoperatively (baseline), and on postoperative days 1 and 3. Comparisons of the two groups based on factors that affect kidney and liver function during surgery were performed by measuring the perioperative fluid volume, urine output, and anesthesia time. The two groups were equally given 1 g amoxicillin (Augmentin™, Ilsung, Korea) twice a day for five days and 90 mg diclofenac (Neufenac™, Ajoo, Korea) twice a day for one day.
The data are presented as the mean ± standard deviation, and statistical analysis was performed with PASW Statistics 18 (Predictive Analytics Software; SPSS Inc., Chicago, IL, USA). Comparisons between the patient characteristics, perioperative fluid administration amount, urine output, and anesthesia time were performed using unpaired t-tests. Comparisons between liver and kidney function within each group and between the two groups were done by repeated measured ANOVA. P < 0.05 was considered statistically significant.
Results
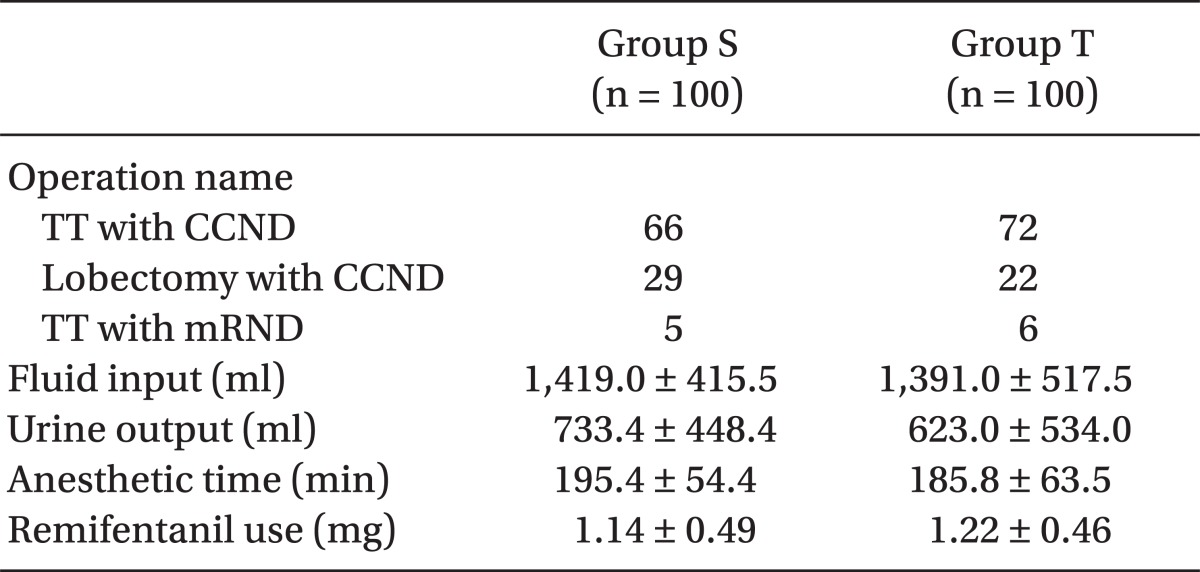
There were no differences between the two groups in type of thyroidectomy, perioperative fluid volume, urine output, amount of blood loss, anesthesia time, and amount of remifentanil used (Table 2).
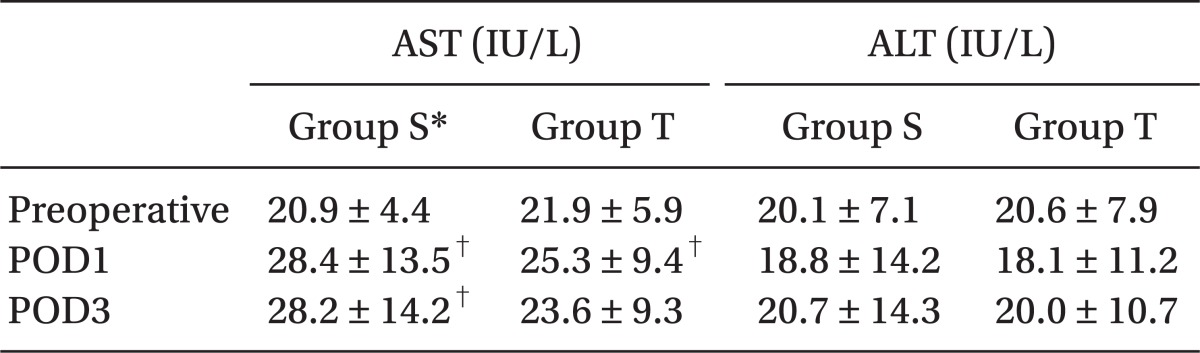
The AST levels in Group S significantly increased on postoperative day 1 (28.4 ± 13.5, P < 0.001) and day 3 (28.2 ± 14.2, P < 0.001), compared to baseline (20.9 ± 4.4). The AST levels in Group T significantly increased on postoperative day 1 (25.3 ± 9.4, P < 0.001), compared to baseline (21.9 ± 5.9) (Table 3). Between the two groups, Group S had a significantly higher AST level than did Group T (P = 0.048), but AST levels in both groups were within the normal range. The numbers of patients who had postoperative AST greater than 40 IU/L were 14 in Group S and 7 in Group T, but there were no significant differences between the two groups (P = 0.083). There were no cases in which AST increased above 100 IU/L.
There were no changes in ALT after anesthesia in either group, and there were no differences between the two groups (Table 3). The numbers of patients who had postoperative ALT greater than 40 IU/L were 4 in Group S and 4 in Group T.
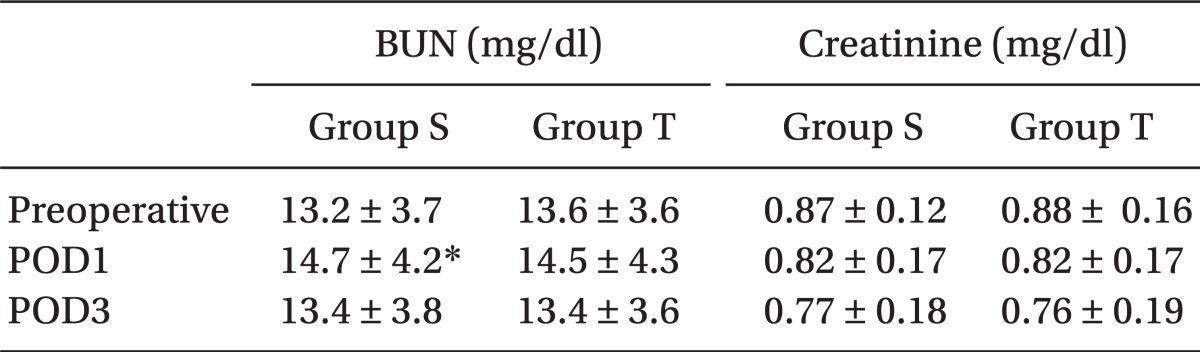
The BUN levels in Group S increased significantly on postoperative day 1 (14.7 ± 4.2) (P = 0.008), compared to baseline (13.2 ± 3.7), but was in the normal range. The BUN levels in Group T did not change postoperatively and there were no differences between the two groups (Table 4). BUN levels outside of the normal range occurred in 1 patient in Group S on postoperative day 1 and in 2 patients on postoperative day 3. In Group T, there was 1 patient with BUN levels out of the normal range on postoperative day 3. There were no changes in serum creatinine after anesthesia in either group, and there were no differences between the two groups (Table 4).
Discussion
Thyroidectomies are known to not cause direct surgical damage to the liver and kidney. They are also associated with low levels of postoperative pain. The surgical site is usually clean and there is little blood loss, and therefore antibiotic and analgesic use can be reduced. Therefore, the context of thyroidectomies are good for the study of the direct effects of anesthetics [7,8].
To assess liver function, albumin, gamma-glutamyl transpeptidase, prothrombin time, and cholesterol may be tested. AST and ALT levels are also often used as screening tests. AST is found not only in the liver, but also in the heart, kidney, and muscles. Therefore, ALT is a more specific test for the liver. In the present study, postoperative AST significantly increased in Group S compared to that of Group T, but the increased AST values were within the normal range. Neither group exhibited changes in postoperative ALT compared to baseline, and there were no differences in ALT between the two groups. There were no cases of AST and ALT increasing more than 100 IU/L. Therefore, we hypothesized that postoperative hepatic dysfunction was clinically insignificant and there was no difference in hepatic function between the two groups.
Sahin et al. [5] compared the effects of inhalational anesthetics and TIVA on patients with lumbar discectomy, and found that there were no changes in postoperative liver function, and found no differences between the two groups. Their findings agree with the results of the present study. Similarly, studies performed by Yoon et al. [6] and Oh et al. [9] on laparoscopic cholecystectomy patients also agreed with our results, in that they found no differences in liver function after surgery with either inhalational anesthesia or anesthesia with propofol. However, their findings differ from those of the present study because postoperative AST and ALT increased beyond the normal range, perhaps because laparoscopic cholecystectomies are associated with relatively greater risk of liver damage due to traction and the surgery itself, more than lumbar discectomies and thyroidectomies. ALT showed no postoperative changes in the present study and in the study by Sahin et al. However, ALT increased in the studies by Yoon et al. and Oh et al. This may be due to direct surgical damage to the liver rather than the effects of sevoflurane and propofol. However, there have been reports of liver failure after anesthesia with sevoflurane in children and adults who had normal liver function [10,11]. There have also been reports of acute liver failure accompanied with fatty liver in patients who received propofol over long periods of time [12]. Sevoflurane and propofol generally are safe for patients with normal liver functions, but it is necessary to be aware that they can cause liver toxicity.
There is disagreement over whether sevoflurane affects kidney function. Mazze et al. [13] performed a large study and found that sevoflurane does not cause kidney insufficiency. Unlike animals, sevoflurane anesthesia does not affect kidney function in humans because human renal beta-lyase activity is lower than animal renal beta-lyase activity. Beta-lyase is an enzyme that is involved in the change of compound A into the kidney toxin cystein-S-conjugate, and it is found 8-30 times more in rats than in humans [14]. However, considering nephrotoxicity after sevoflurane anesthesia in healthy volunteers [15] and kidney insufficiency after sevoflurane anesthesia [16], further study on the effects of sevoflurane on kidney function are needed.
In the present study we used remifentanil in both groups for anesthesia maintenance. Group S used an infusion pump for continuous infusion. Group T used a TCI pump to control the effect-site concentration. Although the administration methods were different, the remifentanil doses were 1.22 mg and 1.14 mg, respectively, so there was no difference between the two groups. Remifentanil is hydrolyzed quickly by circulating nonspecific tissue esterase. Liver and renal dysfunction found in the perioperative period does not affect opioid pharmacokinetics [17]. Thus, the remifentanil used in the present study is not considered to have affected the postoperative liver or kidney function.
The BUN levels in Group S significantly increased postoperatively. However, the BUN values were in the normal range and there was only a slight change (1.5 mg/dl). Also, a total of 40-50% of BUN is reabsorbed in the renal tubule, and the reabsorption rate increases in the hypovolemic state. If protein metabolism is not stable, it cannot represent the glomerular filtration rate [18]. Thus, it is not considered a clinically significant increase. Creatinine has a tendency to decrease postoperatively. This is considered to be due to dilution from the fluid used during surgery (approximately 1.5 L) and fluid used postoperatively (3-4 L/day). The preoperative hematocrit (40%) decreased to 37% on postoperative day 1. Therefore, considering the small amounts of perioperative blood loss (less than 50 cc), this finding was likely due to the fluid administered in the perioperative period. Urinary glucose and protein, neutrophil gelatinase-associated lipocalin, cystatin C, and interleukin-18 are known to be more sensitive markers [19,20]. In the present study we used BUN and creatinine together to assess kidney function, so our ability to obtain good results was limited. Comparative assessments of kidney function should be made using more sensitive tests.
Liver toxicity is rare with the use of diclofenac, and the short term use of diclofenac does not cause kidney toxicity [21]. However, amoxicillin is known to cause liver and kidney failure, albeit infrequently [22,23]. In the present study, as there were no cases of significant liver or kidney failure, we hypothesized that the drugs (anesthetics and antibiotics) used during anesthesia had no effect on liver or kidney function.
In conclusion, inhalational anesthesia with sevoflurane and TIVA with propofol and remifentanil had little effect on postoperative liver and kidney function, and did not cause clinically significant organ insufficiency in thyroidectomy patients. However, further studies are needed in patients with preoperative liver insufficiency and in patients undergoing liver transplants or surgeries that directly affect liver function, such as hepatic resection.
 XML Download
XML Download