

 PDF
PDF Citation
Citation Print
Print


Introduction
Patient-controlled analgesia (IV-PCA) is a delivery system that allows patients to self administer analgesics, which are predetermined by their physicians, to relieve pain. Since IV-PCA was introduced in the early 1980s [1], it has become widely accepted for the management of postoperative pain. The use of IV-PCA has been increasing because of its proven advantages over conventional intramuscular injections [1]. These include improved pain relief, greater patient satisfaction, less sedation, and fewer postoperative complications. Studies have also demonstrated patient satisfaction with acute pain service (APS) [2].
It is difficult to evaluate IV-PCA using a cost-utility analysis [3], because no universally accepted method of assigning monetary value to transient disutility such as postoperative pain is currently available. Willingness to pay (WTP) means the maximum amount of medical cost a patient is willing to pay to gain benefits or prevent any risks in medical care [4]. WTP is a methodological tool that seeks to estimate the capacity of certain social groups to pay to find out the hypothetical monetary value for programs and specific medical interventions and treatments.
The purpose of this study was to investigate the WTP for IV-PCA and the relationship between characteristics of patients and WTP in Korea.
Materials and Methods
All participants were scheduled for elective surgery under general anesthesia. This trial included patients who were aged 18-80 yrs to undergo various surgical procedures. To conduct regression tests, a power of 0.85 and an effect size of 0.15 were selected. Using these estimates, we decided to include 400 patients as the final sample size. After obtaining approval from the institutional ethical committees and written informed consent, we enrolled 400 adult patients. In the preoperative visit, patients were asked to complete a questionnaire on their WTP of IV-PCA (PCA pump, Ambix Anaplus®, E-Wha Fresenius Kabi, Korea; drugs, fentanyl or morphine/ketorolac) for postoperative pain.
The patient was requested to indicate a series of predefined amounts of money (Korean won; 30,000/50,000/100,000/150,000/200,000/300,000/500,000) that he or she would be willing to pay for reducing the pain as much as possible. We also recorded patient characteristics, such as age, sex, type of surgery (cancer or noncancer), IV-PCA history, education level (middle school graduation or below/high school graduation or dropout/university student or above), the person responsible for medical expenses (self or spouse vs others), type of insurance (National Health Insurance vs Medicaid), net annual income (Korean won; 0/1-12,000,000/12,000,000-46,000,000/more than 46,000,000), and residential area (urban area vs rural area). Three days after the operation, we asked about the degree of satisfaction and the WTP for IV-PCA.
Data were reported as the median value (25-75%) or mean ± SD. To explore multivariate relationships, the chi-square test for preoperative WTP dependence on patient characteristics was performed, and then the Spearman rank order correlation test was performed. The following characteristics were considered as possible covariates for preoperative WTP: age, sex, type of surgery, IV-PCA history, education level, the person responsible for medical expenses, type of insurance, net annual income, and residential area. A linear regression test for dependence of individual WTP changes on IV-PCA experiences and degree of satisfaction were also performed. All statistical analyses were performed by SigmaStat for Windows version 3.1. P < 0.05 was considered to be statistically significant.
Results
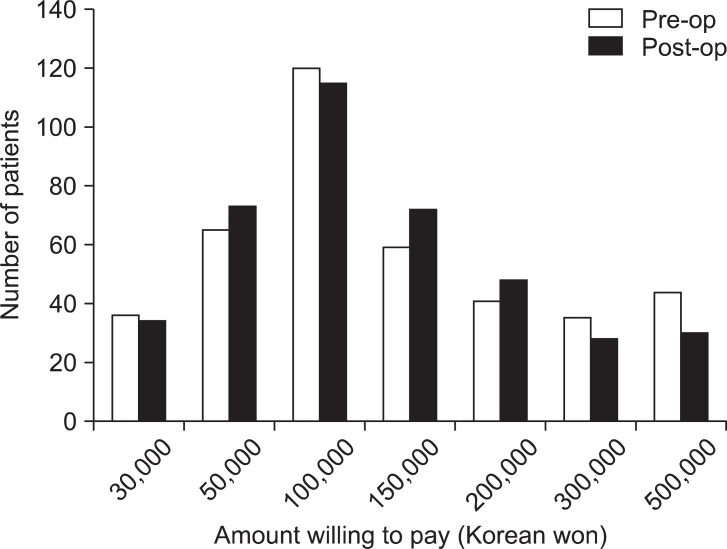
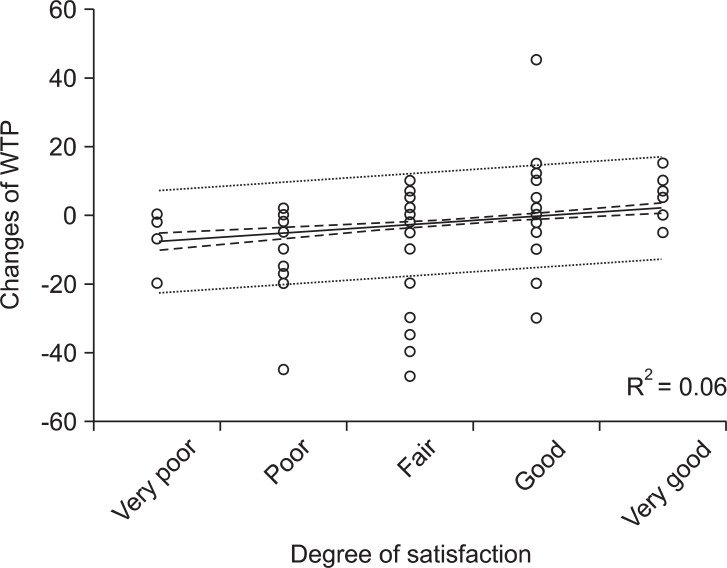
Of the 400 participants, 400 (100%) responded the WTP questionnaire, and complete preoperative and postoperative WTP data for IV-PCA were obtained. The patient's characteristics are shown in Table 1. The mean age was 48.9 ± 13.8 years. Two groups, 0 won (40.2%) and 12,000,000-46,000,000 won (39.8%) consisted of the majority of patients' net annual incomes. For IV-PCA, the number of patients who selected WTP 100,000 won before and after surgery was 120 (30%) and 115 (28.85), respectively (Fig. 1). All patients' characteristics including age, sex, type of surgery, IV-PCA history, education level, the person responsible for medical expenses, type of insurance, net annual income, and residential area were not related to preoperative WTP for IV-PCA. After surgery, 69.0% of the respondents were willing to pay the same amount of money for IV-PCA compared with the WTP before surgery, whereas 18.5% decreased their bid and 12.5% increased their bid. However, the increase in WTP after surgery had a tendency correlated with a higher degree of IV-PCA satisfaction (Fig. 2).
Discussion
IV-PCA has been shown in numerous studies to be beneficial for patients and for relieving pain, but no published studies have investigated cost-efficacy for IV-PCA. In general, the cost of IV-PCA has been decided without patient opinion in Korea. We measured patients' WTP for IV-PCA before and 3 days after surgery. This study showed that the preoperative median WTP for IV-PCA was 100,000 won (25-75%; 50,000-200,000 won). It was not changed even after surgery. The national average cost for IV-PCA was about 120,000-300,000 won, although it varies depending on the specific PCA pump used and the amount or kind of drug administered.
In this study, it was found that increased WTP for IV-PCA had a tendency of correlation with higher levels of patient satisfaction. Those who had higher degrees of satisfaction showed a greater cost from their presurgical bid [5,6]. In the previous study to determine WTP for hip and knee joint replacement surgery, a significant correlation was found between WTP and degree of satisfaction [7]. Therefore, we believe that the degree of satisfaction is sufficient to reflect the degree of analgesic and side effects. We expected that patients who experienced great degrees of satisfaction for IV-PCA would increase their bid after IV-PCA. Although the increased WTP for IV-PCA have a tendency towards higher degrees of satisfaction, the median WTP was not changed before and after surgery.
Previous studies confirm the relationship between income and WTP for postoperative nausea and vomiting (PONV) [6,8-11], but the influence of net annual incomes on WTP could not be confirmed in our study. Other studies showed that income was not significantly correlated to WTP for total knee replacement (TKR) or PONV [7,12]. This result may be due to the fact that almost 70% of the group were pensioners and had limited incomes. In our study, net annual incomes of 43.3% of participants were 0. Although we were not able to confirm that income is significantly correlated to WTP for IV-PCA, patients who earned higher incomes tended to be have a greater WTP without statistical significance.
We also assumed that the estimates for WTP were highly dependent on age, type of insurance, education level, and IV-PCA history. A previous study found that WTP for TKR was correlated with age [7], showing that older respondents undergoing TKR were more likely to be willing to pay. The reason might be that patients in the study suffered from arthritic pain for a long time. However, a significant correlation was not found between WTP and age in our study. Other previous studies found that WTP was correlated with type of insurance [13] or education level [11,14]. Although health care is comprehensive in Korea with almost every therapeutic treatment provided with little cost to patients, the cost of IV-PCA is not covered by the current health care system. A significant correlation between WTP and type of insurance was not found in our study. Education level of the patient was not a predictor for WTP, but patients with higher education levels tended to have more WTP without statistical significance. IV-PCA history was not a predictor for WTP, either.
Our study has several limitations. First, the presentation skills of data collectors can influence the results, which can be introduced with a facilitator bias. Although instructions and scripts were provided to the facilitators, our results still have a facilitator bias because the presentation was given by multiple facilitators. Second, the respondents in this study did pay the full cost of their IV-PCA because National Health Insurance does not cover the cost of IV-PCA in Korea. Therefore, our results may not be generalized to other hospitals in other provinces or cities.
In conclusion, the median WTP for IV-PCA was 100,000 won. The increased WTP for IV-PCA showed a tendency of correlation with higher degrees of patient satisfaction after surgery, but the WTP value may be independent of age, sex, IV-PCA history, education level, the person responsible for medical expenses, type of insurance, net annual income, and residential area.

 XML Download
XML Download