

 PDF
PDF Citation
Citation Print
Print


Introduction
In regional nerve blocks, the use of adjuncts along with local anesthetics can improve the anesthetic effect [1]. Epinephrine and bicarbonate are widely used as adjuncts for regional nerve blocks, because they reduce the onset time and prolong the duration of analgesia. Epinephrine makes local anesthetics last longer by reducing the adjacent blood flow and bicarbonate increases the non-ionized form by alkalinizing the local anesthetics [2].
Bupivacaine and ropivacaine are local anesthetics commonly used in regional nerve blocks. In particular, ropivacaine is known to have less toxicity to both cardiovascular and central nervous systems, compared to bupivacaine [3]. However, even the use of ropivacaine alone reduces the adjacent blood flow; thus, mixing ropivacaine with epinephrine does not have the effect of an adjunct. Furthermore, mixing ropivacaine with bicarbonate may reduce the bioavailability of ropivacaine by causing precipitation [4-7].
Warming of some local anesthetics, e.g. bupivacaine, reduces the pKa values and increases the non-ionized form; therefore, reduced onset time and increased duration can be anticipated in regional nerve blocks, similar to using bicarbonate as an adjunct, as previously reported [8-10].
Changes in the onset time of the sensory and motor block, as well as changes in the duration of analgesia have been recorded after warming ropivacaine to the temperature of 37℃, when performing axillary nerve block.
Materials and Methods
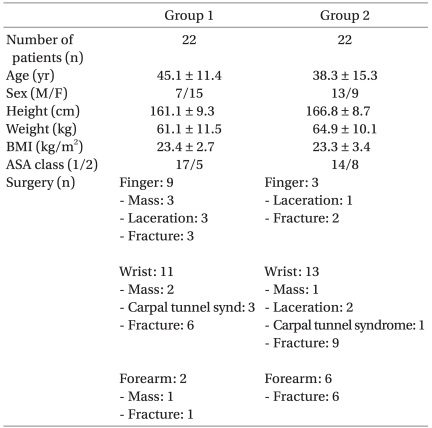
The subjects of this study were 44 patients aged between 18 and 69 years, who underwent upper arm surgery and whose ASA class was 1 or 2 (Table 1). Prior to the study, the patients and their caregivers were given an explanation about this study and signed informed consent forms. Patients with coagulopathy or neurological disorder and those with BMI higher than 35 kg/m2 were excluded from the study. The double blind design could not be used because the doctors had to directly touch and look at the drugs during the experiment.
For patients in Group 1, 30 ml of 0.5% ropivacaine solution were prepared by mixing 20 ml of 0.75% ropivacaine (Rocaine inj®, Reyon pharmaceuticals, Korea) with 10 ml of normal saline, both stored for more than 24 hours in a cabinet in which the temperature was maintained at 20℃; this mixture was used for the axillary nerve block. Before use, the equipment, syringes, and scalp vein needles used for anesthesia were stored in a room in which the temperature was maintained between 20 and 24℃.
For patients in Group 2, 30 ml of 0.5% ropivacaine solution was prepared by mixing 20 ml of 0.75% ropivacaine with 10 ml of normal saline, both warmed up to 37℃; this warmed mixture was used for the axillary nerve block. For the warming of ropivacaine, an air chamber (LD-918H5, lequip, Republic of Korea) was used, which was designed to maintain the temperature at 37℃. We checked that ropivacaine ampoules were maintained at a temperature of 37℃ when stored in the chamber for 20 minutes. The ropivacaine, equipment, syringes, and scalp vein needles used for the axillary nerve block were stored in this air chamber for more than two hours, before the start of the procedure.
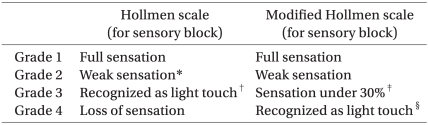
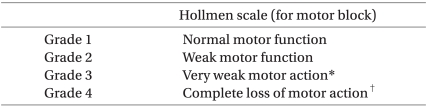
During the axillary nerve block, the pulse at the axillary artery was palpated and the axillary artery was punctured using a scalp vein needle. Ropivacaine was injected four times into the area near the axillary nerve, through repeated artery perforations, with 5 or 10 ml injected each time. After injection, the onset of the sensory and motor block was evaluated six times over a period of thirty minutes, at five-minute intervals. Evaluation of the sensory and motor block was performed individually for the radial, ulnar, median, and musculocutaneous nerves, by a doctor who did not perform the axillary nerve block. Alcohol swab was used to evaluate the sensory nerve block. The cold sensation was compared between the anesthetized and non-anesthetized arm at the same regions innervated by individual nerves. The Hollmen scale was referred to with respect to the onset time of the sensory nerve block. The modified Hollmen scale was applied to increase the objectivity of the record, taking into consideration the time when the grade was 3 or higher for the onset time (Table 2) [11]. For the motor nerve block evaluation, the Hollmen scale was also applied, comparing the movement controlled by the same nerve in both arms (Table 3). The radial nerve was evaluated on the basis of abduction of the thumb and extension of the wrist, the ulnar and median nerves on the basis of the grasp, and the musculocutaneous nerve on the basis of arm flexion. The duration of analgesia was determined as the time from immediately after ropivacaine injection to the time when the patient first demanded injection of an analgesic after the end of operation.
The SPSS software version 15.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Data for statistical analysis showed abnormal distribution, except the duration of sensory nerve block. However, a non-parametric test (i.e. the Mann-Whitney U test) was performed, because the number of subjects in each group was less than 30.
Results
The study was conducted in a total of 44 patients in Groups 1 and 2, with 22 patients in each group. There was no significant difference in the demographic characteristics between the two groups. Anesthesia failed in 2 patients for each group, and these four patients were excluded from the final analysis. No side effects of anesthesia were observed during the perioperative period.
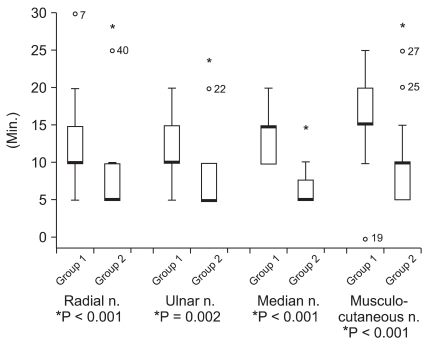
The onset time of the sensory nerve block was significantly shorter in Group 2: by 43% in the radial nerve, by 38% in the ulnar nerve, by 55% in the medial nerve, and by 40% in the musculocutaneous nerve, compared to Group 1 (Fig. 1).
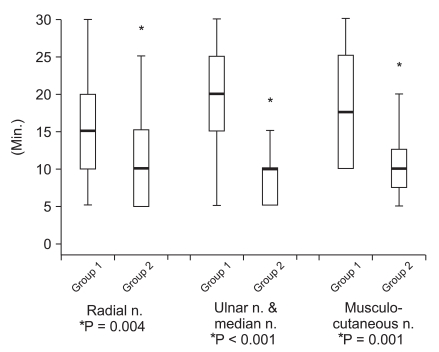
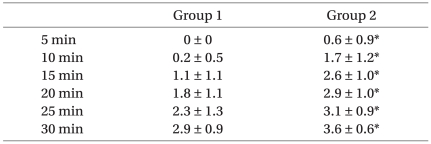
The onset time of the motor nerve block was also significantly shorter in Group 2: by 37% in the radial nerve, by 59% in the ulnar and medial nerves, and by 42% in the musculocutaneous nerve, compared to Group 1 (Fig. 2).
In addition, the number of nerves blocked within 30 minutes after the anesthetic injection was significantly increased in Group 2, compared to Group 1 (Table 4).
The duration of analgesia was 606 ± 186.7 minutes (mean ± standard deviation) in Group 1 and 738 ± 245.5 minutes in Group 2. Although the duration of analgesia was about two hours longer in Group 2, the difference was not statistically significant (P = 0.056).
Discussion
In a short and simple operation at the upper limbs, regional brachial plexus block can be useful. For this purpose, the axillary block is a simple, safe, and reliable approach, and it can be applied to a wide extent in operations at the upper limbs [12,13]. Ropivacaine is a useful local anesthetic for brachial plexus block. Despite the relatively long onset time of regional block, ropivacaine is frequently chosen because of its relatively low toxicity to both cardiovascular and central nervous systems and its relatively long analgesic duration [3,4].
Hydrochloric acid is included in most of the commonly used local anesthetic solutions, to increase the water solubility and to store the solution in a stable state, setting the pH between 4 and 6. Thus, the local anesthetic is mostly ionized in solution. If such a solution is directly used, the onset time of the regional nerve block is longer, because the number of non-ionized species that can pass through the cellular membrane is small. When bicarbonate is used as an adjunct together with ropivacaine, the onset time of the nerve block is shortened, as the number of hydrogen ions is decreased, whereas the number of non-ionized species is increased [1]. Such pH control plays a critical role with respect to the onset time of local anesthetics. This is the reason why opioids with a low pH, such as fentanyl, can hardly be used as an adjunct to enhance the quality of anesthesia [14].
In addition to the use of bicarbonate, warming of the local anesthetic solutions has the effect of increasing the non-ionized local anesthetic species, since it increases the pKa value and the hydrogen ions are separated from the ionized local anesthetic species [8]. It has been reported that shortening of the onset time of the nerve block can be anticipated by an increase in the non-ionized local anesthetic species through warming [9,10].
Several studies have investigated the effect of local anesthetics on various regional nerve blocks. Using bupivacaine and prilocaine in the brachial plexus block, Heath et al. [10] reported that the onset time of the nerve block was shortened by 30% and 50%, respectively, by warming of the local anesthetics, depending on the nerves. Similarly, using ropivacaine in an epidural block, Liu et al. [15] also reported that the onset time of the epidural block was shortened by warming of the local anesthetic, and there were no side effects related to warming. These results can be explained as warming of the anesthetic decreased pKa value and increased permeability through the non-neural tissue to the nerve, which can also support our results [16,17]. However, the basic mechanism for the decrease in the onset time of the nerve block by warming of local anesthetics is still uncertain , and some results were contradictory. Thus, using lidocaine in a brachial plexus block, Chilvers [18] reported that the success ratio of the nerve block was lower in the group for which the local anesthetic was warmed and that there was no difference in the onset time between the two groups when the block was successful. In contrast, in our study, we found that the onset time of both the sensory block and motor block decreased by about 40-50% and the difference between groups was statistically significant.
Similar to our results, using bupivacaine for spinal anesthesia, Beardsworth and Lambert [19] reported that warming of the local anesthetic significantly extended the duration of the sensory nerve block and suggested that the result might have been caused by the decrease in the pKa value of the local anesthesia through warming, although the mechanism was not certain. In our study, the mean duration of analgesia was 606 minutes in Group 1 and 738 minutes in Group 2, indicating that the duration was about two hours longer in Group 2, although the difference was not statistically significant (P = 0.056).
In the literature, there are reports of brachial plexus blocks where warmed bupivacaine, prilocaine, and lidocaine were used; however, to date, there was no study conducted with warmed ropivacaine. In this study, the brachial plexus was blocked with ropivacaine and our results show that the onset time of both the sensory block and motor block decreased by about 40-50% when the anesthetic was warmed.
In conclusion, this study showed that warming of ropivacaine to the body temperature may be clinically applied to shorten the onset time of the regional nerve block.
 XML Download
XML Download