

 PDF
PDF Citation
Citation Print
Print


Congenital tracheal stenosis (CTS) is a rare, but life-threatening condition and the mortality rate is 44-79% [1]. Airway obstruction in patient with CTS could be exacerbated due to spasms, inflammation, or direct trauma after airway manipulation or surgery [2]. In several studies, CTS is associated with other congenital anomalies, especially congenital heart disease (CHD) and tracheal bronchus [3,4]. In infants with congenital tracheobronchial anomalies accompanying CHD, the risk of severe airway obstruction may increase in the perioperative period because of invasive access to the upper airways during intubation and airway manipulation, cardiopulmonary bypass (CPB), or prolonged mechanical ventilation [5]. Associated tracheal bronchus also increases the risk of respiratory complications after endotracheal tube (ETT) intubation [6].
We present a case of CTS combined with CHD and tracheal bronchus to create awareness among clinicians that such a condition could result in severe airway obstruction and prolonged atelectasis in perioperative period.
Case Report
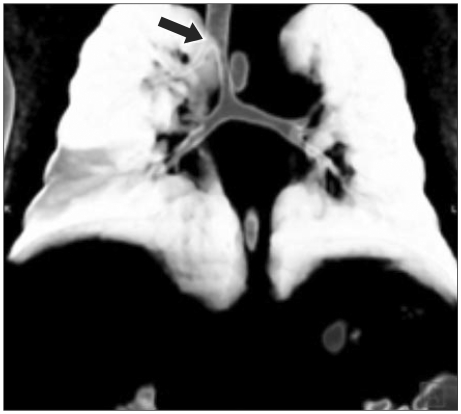
A 3-week-old female patient weighing 3,180 g, was scheduled for total correction of double outlet right ventricle (DORV) with CPB. She was born at the gestational age of 41 weeks from a healthy mother after a normal pregnancy and vaginal delivery; her weight at the time of delivery was 2,800 g. She was hospitalized because of pneumonia of the right upper-lobe (RUL). A heart murmur was detected during a physical examination incidentally. Echocardiography revealed a large perimembranous ventricular septal defect (VSD) with overriding aorta. She was, therefore, referred to our hospital for surgery. During preoperative evaluation, 3-dimensional reconstruction computed tomography (CT) of the thorax revealed stenosis of the trachea and tracheal bronchus (Fig. 1). A tracheal bronchus, with no upper lobe bronchi arising from the right main bronchus, had arisen from the right wall of the trachea 20 mm below the vocal cord. The stenotic lesion had extended from the origin of tracheal bronchus to the carina (length of stenosis was 22 mm), without involving the carina. The luminal diameter at the narrowest of the trachea was 2.4 mm. Although the patient presented with recurrent pneumonia, surgical intervention for tracheal stenosis was not scheduled because her respiratory condition was not compromised by the stenosis. Laboratory investigation revealed no significant findings.
Anesthesia was induced with thiopental sodium (5 mg/kg body weight), fentanyl (3 µg/kg body weight), and rocuronium (0.6 mg/kg body weight). A 3.5 mm uncuffed ETT was placed 5 mm above the tracheal bronchus, and the accuracy of tube positioning was confirmed by using a fiberoptic bronchoscope (BF-N20; Olympus, Tokyo, Japan). General anesthesia was maintained with sevoflurane (end-tidal concentration of 1.0-2.0%) and intravenous infusion of fentanyl (3-5 µg/kg/h), and intermittent bolus doses of rocuronium (0.15 mg/kg body weight). Mechanical ventilation was performed in a pressure-controlled mode with peak inspiratory pressure (PIP), 18-20 cmH2O; respiratory rate (RR), 20-25 breaths/min; end-tidal carbon dioxide (ETCO2), 30-40 mmHg; fraction of inspired oxygen (FiO2), 0.5-1.0, with oxygen saturation (SpO2) ranging from 99-100%. The total correction of DORV was performed uneventfully under CPB. The CPB time was 81 minutes and the operation took 195 minutes.
The patient was transferred to the intensive care unit (ICU). She was put on pressure-controlled ventilation under the following conditions: PIP, 20-23 cmH2O; RR, 20-25 breaths/min; positive end-expiratory pressure, 3-5 cmH2O; ETCO2, 32-55 mmHg; FiO2, 0.4-0.8; SpO2 98-99%. The immediate postoperative course was uneventful. On the first postoperative day (POD), spontaneous breathing trial was performed to discontinuation on mechanical ventilation and early postoperative extubation using T-piece. Significant hypercarbia (PaCO2 was 60-70 mmHg) and tachypnea (RR was 55-60 breaths/min) persisted and the tracheal tube could not be removed. Despite adjustments to increase minute ventilation, there was a gradual increase in end tidal carbon dioxide by 60-70 mmHg on POD #2-3. PIP in a pressure-controlled mode was readjusted from 20-23 cmH2O to 28-33 cmH2O. An arterial blood gas analysis showed pH 7.16; PaCO2, 89 mmHg; PaO2, 124 mmHg; and SpO2, 98% (FiO2 0.8). Chest auscultation revealed reduced breath sounds bilaterally. Plain chest radiography indicated RUL atelectasis (Fig. 2). Fiberoptic bronchoscopy revealed almost complete occlusion of trachea below the tracheal bronchus. The patient was scheduled for surgical repair of congenital tracheal stenosis under slide tracheoplasty using CPB.

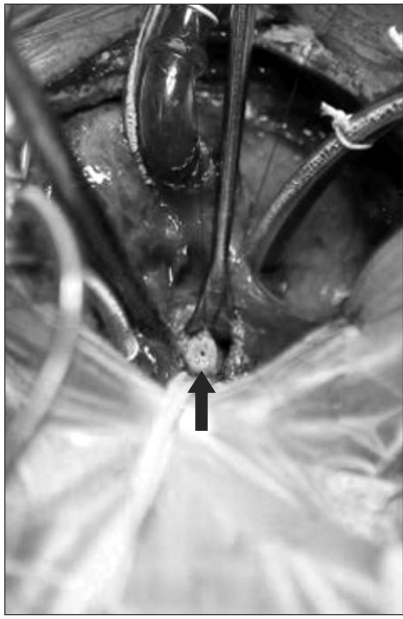
The findings of the preoperative arterial blood gas analysis were as follows: pH 7.01; PaCO2, 115 mmHg; PaO2, 76 mmHg; and SpO2, 93% (FiO2 0.8). Other laboratory investigations revealed no significant findings. Immediately after the induction of general anesthesia, the patient's condition deteriorated rapidly and ventilation was not effective. Arterial blood gas analysis revealed severe respiratory acidosis with CO2 retention of up to 130 mmHg. A median sternotomy was reopened promptly to expose the heart and blood vessels. After the establishment of CPB, CO2 levels were gradually reduced during the bypass period. The ETT was removed and fiberopic bronchoscopy was performed to confirm the extent and degree of stenosis. The trachea was then transected at the narrowest point which inner diameter was 1.0 mm (Fig. 3). Slide tracheoplasty was performed without any complications. Following this, the ETT was repositioned under direct visual guidance and mechanical ventilation was then resumed and CPB withdrawn. At the end of the surgery, the patient was hemodynamically stable.
The patient was transferred to the ICU and placed under pressure controlled ventilation support. On POD #4, a portable chest X-ray showed an improvement in the RUL atelectasis. The endotracheal tube was extubated on POD #7 successfully. She was discharged from the ICU on POD #9. Three-dimensional reconstruction CT on POD #11 demonstrated an almost normal trachea and mild stenosis of the proximal main bronchus, but she did not suffer from any respiratory symptom.
Go to : 
Discussion
CTS is a life-threatening, emergency condition that usually presents very early in life and causes severe respiratory distress. It is a rare anomaly in the general population, but the incidence of CTS in infant with CHD has been reported to be 2.5% [3,7]. A study of multicenter analysis reported that the highest mortality rate was observed in CTS patients younger than 1 month and in those with CHD [8]. Prompt diagnostic evaluation of the airway should be performed in infants with symptoms, such as stridor, episodic desaturation, failure of postoperative extubation, neonatal respiratory distress. Flexible bronchoscopic assessment is safe and useful for evaluation of airway problems complicating congenital heart disease perioperatively [9]. Recently, 3-dimensional reconstruction CT has been recommended for routine evaluation of tracheobronchial anomalies in patient with CHD [4].
The optimal treatment for CTS remains controversial, ranging from conservative therapy to surgical intervention. Conservative management is preferred in infant with mild symptoms as an initial approach. Depending on the size and location of the obstruction, surgical approaches like resection-anastomosis or various forms of tracheoplasty may be considered. Recent studies reported that slide tracheoplasty was a preferred method for long-segmental stenosis [10,11]. And several studies demonstrated that simultaneous repair of CTS and cardiac anomalies is a reasonable surgical approach [12,13]. But staged correction may be considered in infants with long-segment CTS and complex cardiac anomalies because those still remain difficult to treat [5].
Tracheal bronchus is a relatively common airway anomaly. The incidence of tracheal bronchus is approximately 2% [6]. Tracheal bronchus may be asymptomatic or may result in recurrent infections due to the retention of secretions. An anomalous RUL bronchus originating from the trachea, at the level of or above the carina, also increases the risk of complications following ETT intubation. If the ETT insertion is very deep, the retention of secretions and obstruction of the tracheal bronchus by the ETT can contribute to RUL atelectasis. Similar problems have been reported in patients with tracheal bronchus undergoing intubation for anesthesia [14,15].
In our case, congenital tracheal anomalies accompanying CHD resulted in severe airway obstruction and atelectasis during postoperative intensive care. The patient's airway, being very small in diameter, was most vulnerable to further stenosis in the event of a careless minor injury. Airway manipulation, mucosal edema, and inflammation associated with cardiac surgery may also influence the luminal narrowing of trachea. Nevertheless, we performed surgical treatment with staged manner because preoperative expected CPB duration would be long and the patient had long-segment CTS with CHD. But concomitant repair of CTS and CHD should be considered as alternative method. RUL atelectasis could have occurred due to incorrect positioning of ETT and accumulation of secretions. When dealing with a patient with CTS during the perioperative period, one should keep in mind that a serious deterioration of the stenotic airway may occur, even if the stenotic lesion had not been severe enough to be treated in the preoperative period. Also, special attention should be paid to the position of the ETT using chest x-ray or fiberoptic bronchoscopy, especially if the patient has CTS associated with tracheal bronchus.
In summary, CTS with CHD can complicate the routine care of infants in the operating room and the ICU. Infants with significant obstructive airway symptoms require urgent attention. Early recognition and prompt diagnosis of acute airway obstruction may prevent complications associated with airway anomalies. Further, it is very important to select an appropriate surgical procedure and optimal timing for the treatment of CTS associated with CHD.
Go to :
 XML Download
XML Download