

 PDF
PDF Citation
Citation Print
Print


Introduction
Hysteroscopy has been used relatively safely in the diagnosis and treatment of various gynecological conditions [1]. It requires the use of an irrigating fluid to dilate the operating field and to wash away debris and blood. A potential complication of such irrigation is systemic absorption of the fluid to the extent that overt symptoms are produced [2]. Hypervolemia causes hyponatremia, hypokalemia, and hypoosmolality and symptoms such as nausea, vomiting, and mental confusion. Massive absorption can even lead to brain edema, brain herniation, and death. Procedures that cause extended endometrial injury such as myomectomy or hysteroscopic endometrial ablation are more likely to trigger hypoosmolality and hyponatremia [3].
An ideal irrigating solution would be a translucent, non-conducting medium that has a similar osmolality with the serum and causes only minimal side effects when absorbed [4]. Dextran is now less frequently used because of possible anaphylactic reaction, although it provides excellent visualization. Glycine is an endogenous amino acid without an allergic reaction potential; however, it had both direct and indirect cardiotoxic effects in animal studies [5]. Unlike glycine, glucose is a physiological solution that is readily metabolized when absorbed [6], but can cause transient hyperglycemia. An alternative irrigating solution is the 2.7% sorbitol-0.54% mannitol, which theoretically causes fewer potential adverse effects. Sorbitol is metabolized to fructose and glucose and can result in hyperglycemia, whereas mannitol causes an osmotic diuresis which can help maintain effective osmolality.
The aim of this study is to compare 2.7% sorbitol-0.54% mannitol and 5% glucose as an irrigating solution for hysteroscopic myomectomy & polypectomy for the occurrence of hyperglycemia, hyponatremic hypoosmolality, and other electrolyte imbalances.
Materials and Methods
This study received Institutional Review Board approval, and informed consent was obtained from 30 ASA I or II patients undergoing the hysteroscopic procedure. Patient preoperative evaluation included complete medical history and routine laboratory examinations (complete blood count, blood glucose, blood urea nitrogen, creatinine, serum sodium, potassium, osmolality). Patients who had a history of diabetes mellitus, coagulopathy, or renal disease were not included in this investigation. Any patients who had received hypertonic saline, diuretic therapy, plasma products, or blood transfusion before the surgery were also excluded.
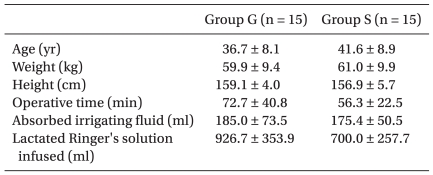
Patients were randomly divided into two groups according to the irrigating fluid used, either 5% glucose solution (Group G, n = 15) or 2.7% sorbitol-0.54% mannitol solution (Group S, n = 15). No significant differences were observed in ages, weights, and heights of patients in either group (Table 1).
Thirty minutes before the surgery, 0.004 mg/kg glycopyrrolate and 0.04 mg/kg midazolam were intramuscularly administered to all patients as premedication. Standard monitoring (electrocardiogram, non-invasive blood pressure, and pulse oximetry) was established in the operating room. All patients were hydrated with a lactated Ringer's solution (8 ml/kg) before the induction; subsequently, the infusion continued with a rate according to the patient's requirements.
Thiopental sodium at 4 mg/kg, 0.8 mg/kg rocuronium, and 1 µg/kg remifentanil were used for induction. Anesthesia was maintained with 0.1 µg/kg/min remifentanil, 1.5-2.0 vol% end-tidal sevoflurane, and controlled ventilation to maintain normocarbia (end tidal carbon dioxide tension between 30-35 mmHg) using fresh gas flow of 3 L/min (60% oxygen).
A preoperative laboratory blood sample was obtained just after the induction (T1). The value of this sample was used as the control value. Irrigating solution was infused by a rotary pump into the uterine cavity under a hydrostatic pressure of 80 mmHg to permit surgical exposure. A two channel, 26-French gauge continuous irrigating resectoscope was used. The gynecologist performed polypectomy and myomectomy with both roller-ball and wire loop electrocautery devices. After 2 L irrigating fluid was infused, an intraoperative laboratory blood sample was obtained (T2), based on the average amount of irrigating fluid used in the hysteroscopic procedure (~4 L) at our institute. The irrigating fluid was collected by passive drainage into a dosed plastic drape, and the amount of the absorbed irrigant was visually estimated by the difference between infused and collected irrigating fluid. The duration of the procedure, the estimated volume of the absorbed irrigant, and the amount of intravenous fluid intake were recorded in each case. A postoperative laboratory blood sample was obtained 1 hr after the end of the procedure (T3).
Statistical analysis was performed using SPSS (version 18.0, SPSS Inc., Chicago, IL, USA). Laboratory measurements of serum sodium, potassium, chloride, glucose, and osmolality between time points within the group were compared using the Kruskall-Wallis test. Data between the two groups were compared using the Mann-Whitney U test. A P value < 0.05 was considered statistically significant.
Results
No significant differences were seen between the two groups in the amount of irrigant absorption and intravenous lactated Ringer's solution intake. During the procedure, there were no hypotensive episodes or surgical complications in any of the patients. Estimated blood loss was minimal in all cases. No patients in either group received blood transfusion.
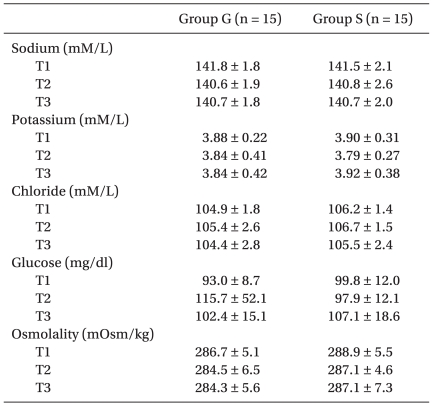
There were no significant differences in the mean value between the studied groups regarding the preoperative serum sodium, potassium, chloride, osmolality and glucose. Furthermore, no significant difference was found in the intraoperative and postoperative laboratory values compared to the preoperative values (Table 2). The mean decrease in sodium concentration intraoperatively (T2) was 1.2 ± 1.4 mM/L in Group G and 0.7 ± 1.5 mM/L in Group S, and sodium concentration had minimal changes postoperatively (T3). The mean blood glucose of Group G was increased by 19.1 ± 48.9 mg/dl while the mean of Group S decreased by 1.26 ± 6.7 mg/dl intraoperatively (T2), but these values were still not significantly different. The mean decrease in serum osmolality was minimal in both groups. In one patient of Group G, a significant elevation in the intraoperative value of blood sugar (295 mg/dl) was observed, which returned back to the normal level 6 hours postoperatively. None of the patients developed ischemic ECG changes. No clinical evidence of hypoosmolality or fluid overload was recognized in either the operating room or the recovery room.
Discussion
Endoscopic surgical procedures, such as transurethral resection of prostate (TURP) and hysteroscopic operation, require continuous irrigating fluid to dilate the operating field and to wash away blood and debris. Irrigating fluid is frequently absorbed directly into the vascular system when a vein has been severed by electrosurgery [2]. Systemic absorption of the irrigating solution may lead to serious complications by pathophysiological mechanisms consisting of pharmacological effects of irrigant solutes, the volume effect of irrigant water, dilutional hyponatremia and brain edema [2]. Large scale fluid absorption is rare but leads to symptoms severe enough to require intensive care.
Several irrigating solutions are available, including sorbitolmannitol, 5% glucose, and glycine. The perfect irrigating fluid is sterile water, but it is probably too prone to well established complications such as hemolysis for routine use. Electrolyte solutions disperse electrical current to decrease the cutting function of resectoscope because of its electrical conducting property. Hence, a hypotonic solution is required during electrocautery resections. A bipolar resectoscope allows resection using normal saline, but vascular overload resulting in pulmonary edema could be expected as a more common problem [7].
Glycine is one of the most commonly used irrigants in TURP, and its intermediary metabolites are known to be cardiotoxic and can cause encephalopathy. The low osmolality (190 mOsm/L) of 1.5% glycine can lead to cerebral edema if largely absorbed [8]. Brain damage with hyponatremia has commonly been related to the magnitude of hyponatremia and the rapidity of decrease in serum sodium level [9].
The 5% glucose solution is physiologically safer than glycine because it is readily metabolized throughout the body when absorbed intravenously; thus, the incidence of complications is lower. Hyperglycemia is a potential problem and appears to be proportional to the duration of surgery [10]. Although 5% glucose during TURP produced immediate postoperative hyperglycemia, it was not associated with electrocardiographic changes in a study performed by Collins et al. [4]. Moghadami-Tabrizi et al. [11] reported that the occurrence of hyponatremia was higher in a patient group with more than a 300% increase from the normal level of serum glucose (7 out of 8) compared to a patient group with less than a 100% increase (1 out of 10) of all patients exhibited hyperglycemia after operative hysteroscopy using 5% glucose.
Although 2.7% sorbitol-0.54% mannitol solution is as equally hypotonic as 1.5% glycine, the osmotic diuretic property of mannitol may maintain the effective osmolality of plasma, which protects against cerebral edema from excess free water. Sorbitol is a natural C6-sugar alcohol found in many fruits. It is metabolized to fructose by sorbitol dehydrogenase in the liver and to a lesser extent in the kidney [12]. Plasma glucose concentration does not rise with a moderate amount of sorbitol intravasation. Trépanier et al. [13] reported a case of massive absorption (approximately 15 L) of sorbitol-mannitol irrigation solution during TURP associated with hyperglycemia and type B lactic acidosis by the metabolism of sorbitol.
In the present study, we did not find hyponatremic hypoosmolality during or after hysterscopic polypectomy and myomectomy using either 2.7% sorbitol-0.54% mannitol or 5% glucose irrigation solution. A non-significant decrease in sodium concentration was observed in both groups, 1.2 ± 1.4 mmol/L in Group G and 0.7 ± 1.5 mmol/L in Group S. The operative time and estimated absorbed irrigant volume was lesser in Group S but not at statistically significant level. In this study, none of the patients in Group G developed severe hyperglycemic symptoms, although one had a serum glucose value of 295 mg/dl after the procedure. The low incidence of transient postoperative hyperglycemia in Group G was not consistent with previous studies [4,14].
Intravesical pressure during TURP does not exceed 22.5 mmHg [15], whereas hysteroscopy requires a higher pressure to distend the stiff uterine walls for visualization of the endometrial cavity. The resection time is longer and the exposed raw surface is greater, so the irrigation solution is more likely to be absorbed during hysteroscopy than TURP [16,17]. According to Hasham et al. [18], the amount of fluid absorbed as assessed by volumetric irrigating fluid deficit and hysterosalpingography was influenced by the intrauterine pressure (IUP) attained during endometrial laser ablation. They found no fluid absorption in a group of 11 women if the mean maximum IUP was 70 mmHg, which is just sufficient to maintain visibility and to prevent bleeding from disrupted vessels. In the present study, the low pressure irrigation of 80 mmHg probably had affected the relatively small clinically estimated irrigation fluid deficit.
Our study was limited by the relatively small size of both patient groups and the small estimated absorbed irrigant volume. We did not see any patients who absorbed enough irrigant to cause complications during the course of this study.
In conclusion, in 30 patients undergoing hysteroscopic polypectomy and myomectomy with mild to moderate absorption of irrigants (average = 180 ml; range = 100 to 500 ml), 2.7% sorbitol-0.54% mannitol and 5% glucose irrigating solution caused no evidence of hyponatremic hypoosmolality or any other electrolyte imbalance. If massive absorption of glucose does not occur in Group G, transient postoperative hyperglycemia seemed to not be an adverse effect. Thus, 2.7% sorbitol-0.54% mannitol and 5% glucose solution as irrigating fluids during hysteroscopic surgery may be treated as nearly equivalent unless massive absorption of fluid occurs.
 XML Download
XML Download