

 PDF
PDF Citation
Citation Print
Print


Introduction
Rocuronium is a commonly used steroidal non-depolarizing neuromuscular blocking agent with a rapid onset of action and an intermediate duration [1]. However, even in unconscious patients during anesthetic induction, rocuronium causes withdrawal movement of the injected hand or arm, or generalized movements of the body after intravenous injection. The major disadvantage of rocuronium is the pain associated with its injection, and generalized movements of the body caused by injection pain may even lead to reflux of gastric contents and pulmonary aspiration [2]. A number of treatment modalities have been recommended in an attempt to reduce withdrawal responses, such as priming technique, local warming at the injection site, pretreatment or mixing with ondansetron, lidocaine, tramadol, fentanyl, magnesium sulphate, sodium bicarbonate, alfentanil and antihistamine [3-8].
Gabapentin is a structural analogue of γ-amino butyric acid (GABA) and was initially introduced as an antiepileptic drug. The drug has also demonstrated antinociceptive, analgesic, and antihyperalgesic properties. Recently it has been used to treat acute and chronic pain after surgery, and to reduce postoperative opioid requirement [9-13].
To our knowledge, a limited number of studies have evaluated the potential influence of gabapentin in general anesthetic induction with rocuronium. This double-blind, randomized, placebo-controlled study aimed to investigate the effects of gabapentin on the incidence and severity of rocuronium injection pain and the changes in hemodynamic variables during anesthetic induction.
Go to : 
Materials and Methods
After obtaining approval from the institutional ethics committee and patients' written informed consent, 86 ASA physical status I or II patients, aged 18-69 years who were scheduled to undergo elective surgery with general anesthesia were enrolled. Exclusion criteria were as follows: patients with ASA physical status III or greater, neurological deficits, pregnancy, anticipated difficult airway, body weight more than 20% of ideal body weight, substance abuse, alcoholism, and those receiving analgesics, sedatives, hypnotics, antidepressants, hemodynamic instabilities during induction. Four patients were dropped from the study. Patients were randomly allocated into 2 groups (43 in each group) with the help of a computer generated table of random numbers to receive either gabapentin 600 mg (Group G) or placebo (Group C) 2 hours prior to surgery.
None of the patients were premedicated, and standard monitoring with electrocardiogram, non-invasive blood pressure, and pulse oximetry was performed. Blood pressure was measured at 1-min intervals. An 18-G intravenous cannula was placed preoperatively in the vein on the dorsum of the hand in the ward and infusion of lactated Ringer's solution was started. Side effects of gabapentin including sedation, nausea, vomiting, somnolence, lightheadedness, dizziness, headache and visual disturbances were recorded before induction. If necessary, symptoms were treated. After 3 min of preoxygenation, 2.5% thiopental sodium 5 mg/kg was injected. When the verbal response and the eyelash reflex were abolished, an intubating dose of rocuronium 0.6 mg/kg was injected over 5 seconds and intravenous fluid was continously administered for 10 seconds. While rocuronium was being injected, withdrawal movement was graded as follows: grade 0 = no response, grade 1 = movement/withdrawal at the wrist only, grade 2 = movement/withdrawal involving the arm only (elbow/shoulder), and grade 3 = generalized response with movement/withdrawal in more than one extremity, cough, or breath-holding [14]. Mean blood pressure (MBP) and heart rate (HR) were recorded before the induction, 1 min before intubation, 1 min and 5 min after intubation.
With reference to the previous study [15,16], the incidence of withdrawal movements was predicted to be approximately 60%, and a 50% reduction in incidence to 30% was considered to be clinically relevant. Power analysis showed that 82 patients were needed for 80% power (β = 0.2) and 95% significance level (α = 0.05) to detect 50% reduction in incidence. 43 patients were enrolled per group assuming a 5% dropout rate. Statistical analyses were performed using SPSS 14.0 for Windows (Statistical Package for Social Science, SPSS Inc, Chicago, IL, USA). Data are expressed as mean ± standard deviation (SD) or numbers (percentages). Discrete variables such as gender, ASA, the incidence of withdrawal movement were analyzed using Chi-square or Fisher's exact test. Student's t-test or Mann-Whitney test were used to compare continuous variables such as age, weight, height, mean blood pressure (MBP) and heart rate (HR) between groups. ANOVA for repeated measures was used to compare the changes in mean hemodynamic variables within the group. A P value of less than 0.05 was considered statistically significant.
Go to :
Results
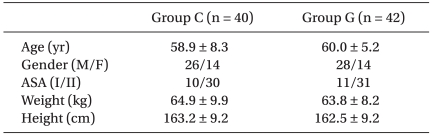
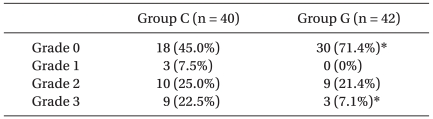
Both groups were comparable with respect to age, gender, ASA status, weight, and height (Table 1). None of the patients in Group G showed gabapentin-related side effects such as sedation, nausea, vomiting, somnolence, lightheadedness, dizziness, headache and visual disturbances before anesthetic induction. The overall incidence (Grade 1-3) of withdrawal movement after rocuronium administration was significantly different between both the groups (55.0% in the Group C vs 28.6% in the Group G, P = 0.02). The number of patients with grade 3 withdrawal response, indicating severe pain, was 9 (22.5%) and 3 (7.1%) in Group C, and Group G, respectively (P < 0.05, Table 2).
Baseline hemodynamic variables were similar between the two groups (Table 3). HR and MBP at 1 min before intubation were significantly lower in Group G compared with Group C. However, HR and MBP at 1 and 5 min after intubation were comparable between the two groups. Comparison of HR and MBP within each group showed significant differences among values with the course of time.

Table 3
Hemodynamic Changes
Values are mean ± SD. Group C: control group, Group G: gabapentin group. Baseline: before induction, Pre-1m: 1 min before intubation, Post-1m: 1 min after intubation, Post-5m: 5 min after intubation, *P < 0.05 compared with group C, †P < 0.05 compared with baseline value within the group, ‡P < 0.05 compared with Pre-1m within the group, §P < 0.05 compared with Post-3m within the group, ∥P < 0.05 compared with Post-5m within the group.
![]()
Go to :
Discussion
The present study demonstrated that pretreatment with a single dose of gabapentin 600 mg 2 hours before surgery significantly reduced the incidence and the severity of withdrawal movement induced by rocuronium administration. Moreover, HR and MBP at 1-min before tracheal intubation were lower in patients pretreated with gabapentin.
The incidence of withdrawal movement associated with rocuronium injection has been reported in 50-100% of patients [15-18]. In our study, the incidence of withdrawal response was 55.0% in the control group. Compared with the previous study, the occurrence of withdrawal movement was comparatively lower in our study. Age and gender play important roles in rocuronium-induced withdrawal movements [19-22]. The overall incidence of rocuronium-induced pain was lower in older patients aged over 65 years compared with that in the young patients aged between 20-40 years in the placebo group [19]. Gender difference in severity and incidence of rocuronium-induced pain also exists in adults [21]. A previous study has suggested that females reported more frequent and severe pain responses than males. Females are considered to be 20-25% more sensitive to rocuronium than males [22]. In our study, mean age of patients in the control group was 58.9 ± 8.3 years and the ratio of females to males was 35%. The relatively low incidence of rocuronium-induced pain may be related with patients' characteristics such as older age and male dominance.
Gabapentin is an antiepileptic drug and a structural analogue of γ-amino butyric acid (GABA). It has been proved to be effective in controlling acute postoperative pain and reducing postoperative opioid requirement [9-13]. In addition, pretreatment with gabapentin attenuated the pressor response to laryngoscopy and tracheal intubation [23]. Gabapentin is not metabolized in humans and its elimination is dependent on renal clearance. The elimination half-life of gabapentin is 5 to 7 hours after an oral dose of 200 to 400 mg. After a single dose of 300 mg, maximum plasma concentration is reached in about 2-3 hours. The bioavailability of a 600 mg single oral dose of gabapentin is about 40% and decreases with an increasing dose. Single dose of 600 mg administered 2 hours before surgery is within the recommended dose limits of 300 to 1200 mg, 3 times a day [24]. It seems to be clinically impractical to use oral gabapentin with a delayed onset of action and a long half-life, for preventing temporary withdrawal movement. However, since patients who were treated with gabapentin before surgery benefited from its influence on maintaining the hemodynamic stability after tracheal intubation and postoperative analgesic effect, pretreatment with oral gabapentin deserves consideration.
Gabapentin is also regarded as a safe drug. It has fewer side-effects and minor interactions with other drugs. Older patients occasionally show increased sensitivity to drugs and doses of gabapentin may be adjusted to their age. We did not observe any adverse effects associated with a dose of 600 mg of gabapentin and it was well tolerated.
Although the exact mechanism of action of gabapentin is unknown, proposed mechanisms are as follows: its ability to increase the concentration and the rate of GABA synthesis in the brain; bind with high affinity to binding sites in brain tissues that are associated with auxiliary subunit of voltage-sensitive calcium channel (α2δ subunits); reduce the release of monoamine neurotransmitters; inhibit voltage-activated sodium channels; and increase serotonin concentration in human blood [25,26]. The drug inhibits voltage-gated calcium channels in the membrane and acts in a similar way to calcium channel blockers [27]. Calcium channel blockers have shown antinociceptive effects in animals [28]. Miranda et al. suggested that a substance with a calcium channel blocking effect should probably have some antinociceptive properties. We speculated that the calcium channel blocking property of gabapentin might also have alleviated HR and MBP before tracheal intubation in the gabapentin group.
In conclusion, pretreatment with a single oral dose of 600 mg gabapentin attenuated the incidence and severity of withdrawal movement after rocuronium administration. The dose used in this trial well tolerated and the patients did not manifest any side effects. Further studies may be needed to investigate the appropriate dose of gabapentin and compare gabapentin with other treatment modalities for preventing withdrawal movement related to rocuronium injection.
Go to :
 XML Download
XML Download