

 PDF
PDF Citation
Citation Print
Print


Introduction
Laryngeal mask airway (LMA) has become an indispensable airway management tool in anesthetic practice. Although it is less invasive than endotracheal intubation, inadequate depth of anesthesia may lead to complications such as airway hyperreactivity or physical injury to the patient [1]. On the other hand, excessive anesthesia carries a risk for developing hypotension or bradycardia [2].
An indicator should give precise information about anesthetic depth to avoid complications owing to deep or light anesthesia, and it should be a simple, repeatable, and accurate maneuver to perform. The weighted syringe drop from the patient's hand [3], verbal command [4], and jaw thrust maneuver [5] were found to be potential indicators of the optimal anesthetic depth for LMA insertion in adults. However, these maneuvers did not provide information about sufficient anesthetic depth for LMA insertion. An alternative indicator such as trapezius squeezing test has been suggested as a useful indicator for LMA insertion in children [6].
The purpose of this study was to compare the effectiveness of the trapezius squeezing test with that of the jaw thrust maneuver as clinical indicators of an adequate condition for LMA insertion in adults under sevoflurane anesthesia.
Materials and Methods
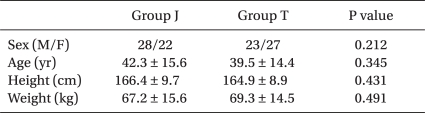
This study was approved by our Institutional Ethical Research Board. Written informed consent was obtained from all patients. We enrolled 100 patients (aged 19-58 years) with ASA physical status I or II undergoing minor surgical procedures such as orthopedic or urologic surgery (Table 1). Patients were randomly assigned to be tested with the trapezius squeezing test (group T, n = 50) or with the jaw thrust (group J, n = 50) using random numbers in sealed envelopes. Patients with asthma, acute respiratory infection or those expected to have a difficult airway were excluded from the study.
Routine anesthetic monitors were attached to the patients on arrival at the operating room. Glycopyrrolate (0.004 mg/kg, IV) was administered to decrease oral and tracheal secretions. Anesthesia was induced via a face mask with a semi-closed circuit system primed with 6% sevoflurane and ventilated with 6% sevoflurane in oxygen with 4 liter/min fresh gas flow. Spontaneous ventilation was first assisted and then controlled manually to maintain an end-tidal carbon dioxide partial pressure of 33-40 mmHg. No neuromuscular blocking agent was used.
Trapezius squeezing or jaw thrust was performed from one MAC (minimum alveolar concentration) of end-tidal sevoflurane concentration according to the study group. The test was repeated every 10 seconds. The trapezius squeezing test was performed by squeezing the trapezius muscle with a squeezing power of 68.6 kg/m/sec2, as gauged by a pinch meter (Green Medical, Palo Alto, CA) and observing motor response. In group J, The jaw was thrust gently by lifting the angles of the mandible vertically upward. A Classic LMA™ (Intavent Orthofix Ltd., Maidenhead, UK) was inserted immediately after a negative response to trapezius squeezing or jaw thrust tests. Motor responses were observed by an independent researcher who waited outside the operating room while the test was performed. Development of coughing, gagging, breath-holding, laryngospasm, SpO2 < 90% or gross purposeful movements during or within one minute of LMA insertion were regarded as unsuccessful attempts. Effective ventilation was determined by observing chest wall movement, auscultation, and capnography.
The insertion time was measured from sevoflurane administration to the negative trapezius squeezing test or jaw thrust. The end-tidal sevoflurane concentration was recorded when the trapezius squeezing test or jaw thrust turned negative. The blood pressure and heart rate were recorded in the preanesthetic preparing room, immediately after the test, and immediately after LMA insertion.
Based on a previous study [6], we calculated the minimum sample size needed to achieve significance to be between 80% and 50% success rates at a level of P < 0.05 and power of 0.8 and determined that 45 patients were needed. Student's t-tests and chi-square tests were used for data analysis. Analysis of variance with repeated measures was used to compare hemodynamic data. Statistical calculations were performed using SAS 8.01 (SAS institution Inc., Cary, NC).
Results
Fifty patients in each group were recruited and no one was excluded from this study. There were no differences in patient characteristics between the two groups (Table 1).
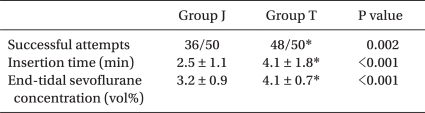
The LMA insertion profile is listed in Table 2. The incidence of successful attempts were 48/50 (96%) and 36/50 (72%) in group T and group J, respectively. It was significantly higher in group T compared to group J (P = 0.002). One patient in group T and 10 patients in group J showed movement of the extremities. One patient in group T and 4 patients in group J required a second LMA insertion attempt due to failure of the mouth to open, or coughing. They ventilated well with an LMA after a second attempt.
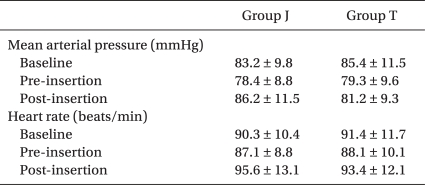
The insertion time for group T was longer than group J (P < 0.001). The end-tidal sevoflurane concentration in group T was higher than for group J (P < 0.001). No significant changes in mean arterial pressure or heart rate were observed in either group at pre- and post-LMA insertion compared to baseline (Table 3).
There were no complications such as laryngospasm, hypoxia, or recall of the pain from the trapezius squeezing test or jaw thrust.
Discussion
This study demonstrates that the trapezius squeezing test is a better indicator of an adequate condition for LMA insertion than the jaw thrust maneuver in adults under sevoflurane anesthesia.
Although LMA insertion requires lighter anesthesia compared to endotracheal intubation, LMA insertion without a neuromuscular blocking agent may induce airway complications such as coughing, gagging, or laryngospasm. In a previous study, apnea, jaw relaxation, loss of verbal contact, and eye lash reflex were suggested as clinical markers for LMA insertion [7,8]. However, these methods had a high incidence of coughing, gagging, hiccups, aspiration, and second trials [7,8].
The jaw thrust maneuver is used frequently in the management of a difficult airway [9]. It is also used as a clinical indicator for LMA insertion because it gives an intense stimulus to anesthetized patients, which allows anesthesiologists to assess patient's anesthetic status. Drage et al. [5] reported a jaw thrust as an adequate clinical indicator to assess the depth of anesthesia for LMA insertion with an 87% success rate, which was slightly higher than that in this study (72%). The difference in LMA insertion success rate assessed with jaw thrust between Drage's report and our manuscript is caused by the presence of an induction agent. Propofol generally decrease the incidence of coughing, gagging, and airway irritation [10]. Response to a jaw thrust led to a higher success rate than other previous studies [3,7], but the incidence of laryngospasm or hypoxia (SpO2 < 90%) was 1.7% and 6.6%, respectively [5]. This may have resulted from the presence of an induction agent in this study.
The trapezius squeezing test, which is performed by squeezing the trapezius muscle and observing movement of the first toe, is negative in deep anesthesia [11]. It has been used as a standard stimulus to assess anesthetic depth. A positive trapezius squeezing test requires more anesthetic to eliminate responses by noxious stimuli. Trapezius squeezing is considered to be a less noxious stimulus than skin incision or laryngoscopy [11]. Based on the end-tidal concentration of volatile anesthetics, LMA insertion is a weaker noxious stimulus than a skin incision [12,13]. For children, the trapezius squeezing test was a reliable indicator for LMA insertion with 91% success rate and a high level of safety [6].
The end-tidal sevoflurane concentration where the trapezius squeezing test becomes negative was 4.1 vol% in adults. This is slightly higher than the 3.6 vol% seen in children [6]. This can be explained by the lack of a hypnotic agent in this study. The end-tidal sevoflurane concentration at which the trapezius squeezing test becomes negative was higher than it was for the jaw thrust maneuver. This suggested that the jaw thrust maneuver is not enough of a stimulus to assess anesthetic depth for safe LMA insertion. The insertion time from inhalation induction to LMA insertion when guided by the trapezius squeezing test was 4.1 minutes. It is resulted from a low flow rate and inspired sevoflurane concentration in order to detect the precise turning point to a negative trapezius squeezing test and jaw thrust maneuver. However, mean arterial pressure and heart rate were maintained during LMA insertion in both groups. These results suggest that the trapezius squeezing test is not an excessive noxious stimulus that can induce hypotension and bradycardia.
In conclusion, the trapezius squeezing test should be used as an indicator of an adequate condition for LMA insertion in adults under sevoflurane anesthesia because its success rate is higher than that of the jaw thrust maneuver, and is without complications.
 XML Download
XML Download