

 PDF
PDF Citation
Citation Print
Print


Introduction
Spinal anesthesia is the most common regional anesthesia conducted for many surgical procedures. Compared to general anesthesia, spinal anesthesia has lower rates of venous thromboembolism, myocardial infarction, requirements of postoperative analgesia, sympathetic responses to surgical stimulation, and several other complications [1-3]. However, complications occurring during or after anesthesia and discomfort from the procedure, position, and neuraxial block may lead patients to prefer general anesthesia.
Because researching patient satisfaction helps evaluate medical care and leads to improved quality of anesthesia, anesthesiologists' attempts to reduce the complications of spinal anesthesia, which can affect the dissatisfaction with spinal block, are extremely important [3-5]. These attempts will also improve the quality of anesthesia and intensify the relationship between anesthesiologists and their patients [4].
To improve the quality of spinal anesthesia, this study was undertaken prospectively to find factors causing dissatisfaction and future refusal of spinal anesthesia.
Materials and Methods
After obtaining the approval of the Ethics Committee at the authors' institution and informed consent, 1,197 patients undergoing elective surgery under spinal anesthesia were recruited over a period of a year, beginning in December 2007. Patients with neurological diseases, psychological disorders, coagulation defects, and spinal anesthesia failure were excluded from the study.
Before attempting spinal anesthesia, attending residents and staff recorded the patient's personal data, such as sex, age, weight, height, previous anesthesia experience, the presence of backache before anesthesia, and the patient's position during the operation. They also collected data about anesthesia, which included the grade of the performer, the needle size, the puncture site and approach, the number of attempts, the neurologic symptoms at the puncture site, the highest level of sensory block, and whether the anesthesiologist succeeded in puncturing appropriately. Spinal anesthesia was administered with 0.5% heavy bupivacaine combined with fentanyl 0-20 µg. Before performing spinal anesthesia, loading of normal saline from 500 ml to 1,000 ml was done to prevent hypotension. Intraoperative complications, including nausea/vomiting, hypotension, bradycardia, inadequate anesthesia/analgesia, and dyspnea were recorded. All authors defined hypotension as systolic blood pressure less than 100 mmHg or below 30% of the initial systolic blood pressure and defined bradycardia as a heart rate below 60 bpm.
On the day after surgery, trained anesthesia personnel visited the patients and collected postoperative data, including postoperative nausea and vomiting (PONV), urinary catheterization due to urinary retention, postoperative backache, postdural puncture headache (PDPH), and transient neurologic symptom (TNS). The patients were also asked about their general satisfaction with spinal anesthesia, causes of dissatisfaction, and causes of their refusal to have spinal anesthesia again.
Statistical analyses were performed using SPSS Software (Version 18.0, SPSS Inc., IL, USA). Data are expressed as a median (range) or number (%). Associations of categorical variables with patient dissatisfaction and refusal were assessed using chi square tests. A univariate odds ratio (OR) and a 95% confidence interval were used as estimates of the risk of categorical variables. Significant (P < 0.05) variables were then entered into multivariate logistic regression models to calculate the adjusted OR. A two-sided P value of < 0.05 was used for statistical significance.
Results
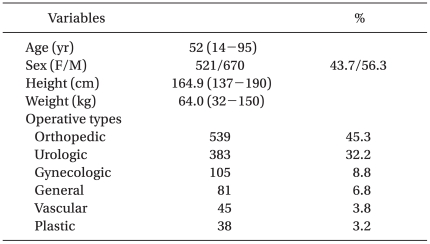
The information on 1,191 patients was entered into the database. Six patients were excluded from the study because of spinal anesthesia failure. Table 1 shows the characteristics and type of surgery of the study population.
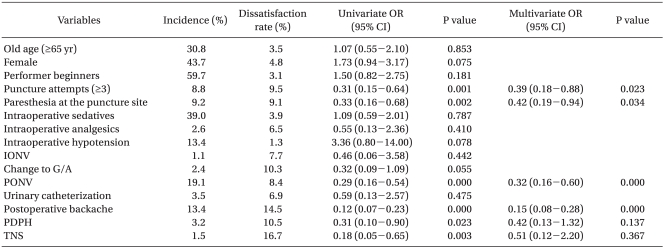
Forty four patients (3.7%) revealed dissatisfaction with spinal anesthesia. Reasons for the dissatisfaction were: backache (29.5%), PONV (20.4%), pain at the puncture site (15.9%), inadequate analgesia (13.6%), consciousness during operation (6.8%), PDPH (4.5%), TNS (4.5%), and urinary retention (4.5%). Table 2 shows the univariate and multivariate analysis for risk factors of dissatisfaction. More than three attempts at a spinal block, paresthesia at the puncture site, PONV, and postoperative backache were the risk factors with P < 0.05.
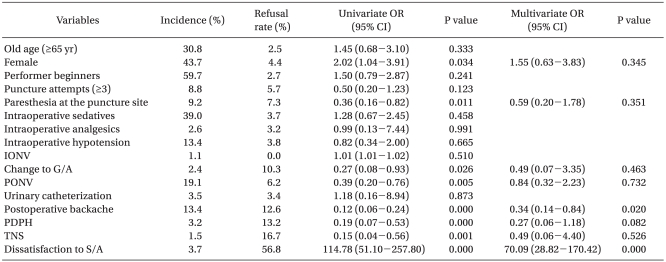
There were 1,153 patients (96.8%) who would opt for spinal anesthesia in the future. Thirty eight patients who refused to receive spinal anesthesia for a similar surgery again revealed several causes for their refusal: fourteen patients (36.8%) disliked being conscious during the operation; ten patients (26.3%) had postoperative backache; five patients (13.1%) had PONV; three patients (7.9%) had PDPH; two (5.3%) had inadequate analgesia; two (5.3%) had TNS; one patient (2.6%) had pain at the puncture site; and one patient (2.6%) had urinary retention (Table 3). In univariate analysis, refusal was associated with females, paresthesia at the puncture site, changes to general anesthesia, PONV, postoperative backache, PDPH, TNS, and dissatisfaction. However, in multivariate analysis, postoperative backache and dissatisfaction itself were the sole risk factors associated with refusal.
Discussion
Researching patient satisfaction is important in understanding problems that patients experience from spinal anesthesia, and it informs improvements in healthcare and the quality of anesthesia. In this study, the dissatisfaction rate of spinal anesthesia was 3.7%, and the refusal rate was 3.2%. Most satisfaction studies of regional anesthesia reported high levels of satisfaction, as shown here. Siddiqi and Jafri [6] demonstrated a high level of satisfaction (83.0%) and the desire to opt for spinal anesthesia in the future (53.7%) among patients receiving spinal anesthesia for caesarean deliveries. Dissatisfaction rate and refusal rate were 3.8% and 6.7%, respectively in Charuluxananan et al.'s study [7]. In Choi et al.'s study [3], 31 out of 194 patients (16%) would reject receiving spinal anesthesia if they had a chance to have it again. Sindhvananda et al.'s study [8], which compared maternal satisfaction between epidural and spinal anesthesia, revealed 90.0% satisfaction in the spinal group. A dissatisfaction rate of less than 15 percent was reported from other surveys on regional anesthesia [6]. Although most studies show a high satisfaction level for spinal anesthesia, the satisfaction rate can be overestimated because patients like to please staff and to meet social expectations by replying "satisfied" [4,6,8].
We found that more than three puncture attempts, paresthesia at the puncture site, PONV, and postoperative backache were predictable factors for dissatisfaction with spinal anesthesia. Charuluxananan et al.'s study [7] also reported that increasing the number of spinal blocks was associated with dissatisfaction. Patients with lower satisfaction scores with spinal anesthesia in the study of Siddiqi and Jafri [6] complained of a higher frequency and severity of postoperative backache. Unlike these studies, Sindhvananda et al. [8] and Bhattarai et al. [9] showed a different main cause for dissatisfaction. Sindhvananda et al.'s study [8] showed that PDPH, pruritus, and PONV were predictors of dissatisfaction. In their study, pruritus was caused of intrathecal morphine [8]. However, we did not use morphine and did not observe pruritis. The main cause of discomfort from regional anesthesia in Bhattarai et al.'s study [9] was immobility of lower limbs. Before spinal anesthesia was performed in this study, symptoms like transient paralysis, numbness, and transient sensory loss in the lower extremities due to the spinal block were explained to patients. Therefore, patients might not have considered immobility of lower limbs as dissatisfaction.
In this study, the risk factors for the refusal to have spinal anesthesia again were postoperative backache and dissatisfaction itself. Also, in Charuluxananan et al.'s study [7], a low satisfaction score of spinal anesthesia care was associated with the refusal of spinal anesthesia. Adjusting modifiable factors related to the dissatisfaction of spinal anesthesia may increase the acceptance of regional anesthesia for similar surgeries in the future. Choi et al.'s study [3] also demonstrated postoperative backache as a risk factor associated with refusing spinal anesthesia in the future. Reducing the number of attempts and having the procedure performed by skilled anesthesiologists reduces the incidence of postoperative backache. Paresthesia of the lower extremities, needle type, and PONV were other causes for refusal in their study.
Postoperative backache was commonly associated with satisfaction and the refusal of spinal blocks, even though the backache may not be directly related to the spinal block [10]. Other variables, such as positioning during surgery, a tightly applied cast or surgical dressing, surgical trauma, operation time, age, pregnancy, needle type, and the number of punctures can contribute to postoperative backache, making it difficult to distinguish the actual cause of back pain [3,10]. We also found that attempting a spinal block more than three times differentiated the satisfied and dissatisfied groups: 105 out of 1,190 patients had more than three attempts made, with 9.4% dissatisfaction with spinal block. Choi et al.'s study [3] demonstrated that the number of punctures was a statistically meaningful factor for the refusal of spinal blocks. However, Schwabe and Hopf [11] reported that backache after a spinal block was not associated with patient characteristics or technical factors, but rather exclusively with pre-existing back pain.
This study may have several limitations. First, when trained personnel or anesthesiologists who performed the procedure asked patients about satisfaction, they usually started with an affirmative question. For example, they asked the patients: "Are you satisfied with spinal anesthesia?". They did not ask: "Are you not satisfied with spinal anesthesia?". Because patients like to please the staff and to meet social expectations by replying "satisfied," patients might have the tendency to answer the question more optimistically. Second, because the trained personnel, who visited patients on the day after surgeries, changed frequently, there may be subjective changes in their assessment of patient responses. Third, to control possible variations, it might be better to have protocols for treatments of intraoperative and postoperative complications, such as hypotension, nausea & vomiting, and pain. Fourth, as patients were interviewed within 24 hours from the spinal block, PDPH occurring after 24 hours from the procedure was not included in the database. PDPH usually occurs within 3 days of the procedure [12] and could be underestimated, which might affect dissatisfaction and refusal rates.
As assessment of patient satisfaction is associated with multiple factors, it is not easy to confirm the variables related to satisfaction. We address this concern by using a large study population and a multivariate logistic regression model. Side effects, such as postoperative backache, inadvertent mistakes, and unskillful techniques, can negatively affect patient perspectives about spinal anesthesia, attending anesthesiologists must perform the procedure carefully and always pay attention to their patients. They must also explain how they will perform the procedure, symptoms after the puncture, and possible complications of spinal anesthesia. Whenever they are faced with difficult cases, it is better to get help or advice from senior staff.
In conclusion, although spinal anesthesia was conducted safely during the study and revealed a high rate of patient satisfaction (96.3%), side effects still occurred. Its risk factors were more than three puncture attempts, paresthesia at the puncture site, postoperative nausea & vomiting, and postoperative backache. The refusal rate to have spinal anesthesia again was 3.2%, and its risk factors were postoperative backache and dissatisfaction.
 XML Download
XML Download