

 PDF
PDF Citation
Citation Print
Print


Epidural space injection is a useful treatment for lumbar radicular pain syndromes. The transforaminal approach has been preferred over the conventional interlaminar method for the diagnosis and treatment of radicular pain; this is because this method provides medicine directly to the intervertebral foramen, at the origin of the irritated nerve. In this manner, the medicine is delivered closer to the nerve root and the anterior epidural space, which maximizes the effects of the treatment [1]. The transforaminal epidural injection (TFEI) is always performed under fluoroscopic guidance in order to confirm the needle position and contrast patterns and visualize the anatomical configuration of the neural foramen. However, treating patients that have developed degenerative changes and have undergone spinal surgery may cause technical challenges in approaching the target region [2]. The occurrence of an intradiscal injection is a potential complication of the TFEI; however, reports of such cases are rare. Here we report an inadvertent discogram where a needle could not be advanced into the intervertebral disc under fluoroscopic guidance during TFEI in the lumbar spine.
Case Report
Case 1
A 61-year-old female patient was admitted to the hospital for evaluation of pain that radiated to the left L5 dermatome, hypoesthesia, and numbness of the legs during walking. These symptoms began two years ago, and a herniated disc on MRI was identified. The patient had pharmacotherapy and physical therapy without improvement. When the patient presented to our service she was diagnosed with a radiculopathy and TFEI was the planned treatment. The infrapedicular approach reported by Bogduk et al. [9] was planned; the L5-S1 TFEI was performed successfully (Fig. 1, 2), and the patient's condition improved significantly over the next 10 days. However, the patient still reported numbness of the legs and therefore an additional procedure was required. In the same manner, after the patient was placed in the prone position and skin disinfectant was applied, the insertion site was covered with a sterile dressing. Using a C-arm fluoroscope (Zen3090®, Zenoray, Korea) to ensure the proper location of the needle tip, local anesthesia was provided with 1% lidocaine. Using a 10 cm long, 22 G, Tuhoy needle, we advanced a block needle to the 6-o'clock position at the L5 pedicle on the oblique view and stopped the advancement before reaching the posterior surface of the vertebral body on the lateral view, after we felt the needle traverse the ligament in the foramen. The needle location was confirmed, but there was no blood or CSF collected by suction. Then, 1 ml of contrast medium (Lopamiro 300®, Ilsung, Korea) was injected in order to perform an epidurogram, when a discogram was confirmed (Fig. 3, 4). No further medication was injected and the block needle was removed. Thereafter, antibiotics were administrated to prevent discitis and oral antibiotics were prescribed for three days. The postoperative visits, in the outpatient department, on days three and seven showed no sign of infection.
Case 2
A 33-year-old male was admitted to the hospital for the treatment of lower back pain; the pain radiated to the right L4 dermatome. The straight leg raising test showed pain at 45 degrees, in the right leg, and the femoral nerve stretch test showed a positive response. Before admission to the hospital, the patient was diagnosed with a herniated disc on MRI, performed at another hospital. He was receiving drug treatment and physical therapy, but his condition did not improve.
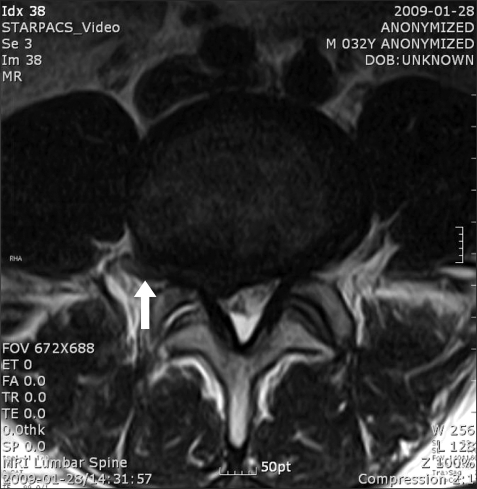
The patient was diagnosed with a radiculopathy and a L4-5 TFEI was performed by the infrapedicular approach. After the patient was placed in the prone position and skin disinfectant was applied, the insertion site was covered with a sterile dressing. Using the C-arm fluoroscope (Zen3090®, Zenoray, Korea) to ensure the proper location of the needle tip, local anesthesia was provided with 1% lidocaine. A 10 cm long, 22 G block needle was advanced to the 6-o'clock position at the L4 pedicle on the oblique view and the advancement was stopped before it reached the posterior surface of the vertebral body on the lateral view, after we felt the needle pass through the ligament in the foramen. The needle location was confirmed, but no blood or cerebrospinal fluid was collected by suction. Then, 1 ml of contrast medium (Iopamiro 300®, Ilsung, Korea) was injected in order to perform an epidurogram, when the appearance of a discogram as well as an epidurogram was noted (Fig. 5, 6). Antibiotics were administrated to prevent discitis, and oral antibiotics were prescribed for three days. Thereafter, an MRI revealed a right foraminal disk herniation at L4-5 (Fig. 7, 8).
Discussion
TFEI is known for its effectiveness in delivering medication to the anterior surface of the epidural space. Using this approach, pain caused by inflamed spinal nerves can be controlled by allowing the medicine to infiltrate the irritated region between the posterior surface of intervertebral disc and the anterior surface of nerve root [1].
The TFEI is always performed under fluoroscopy guidance to confirm the needle location and contrast images. When there are morphometric changes or displaced tissues, not shown on the fluoroscopic view, such as a herniated disc, this procedure may cause damage to tissue. In fact, intradiscal injection during TFEI can occur. However, such reports are rare; there are no previous cases reported in Korea [3-5].
In cases 1 and 2, although the block needle location was determined to be appropriate during the TFEI procedure, for these patients with a herniated disc, a discogram was confirmed by the contrast patterns using fluoroscopy. Manchikanti et al. [6] reported that the disc changes in patients that underwent the TFEI procedure included disc bulging in 42% of the cases, disc herniation in 39%, and regressive changes in 42%.
Park et al. [7] reported that lateral disc herniation (foraminal herniation or herniation protruding into the lateral neural foramen) was responsible of 1-11.7% of all lumbar disc herniations, and that among the patients with lateral disc herniation, 3.4% occurred in L1-2, 14.4% in L2-3, 33% in L3-4, 33% in L4-5, and 16.9% in L5-S1. In addition, Lee at al [8] reported that 4.3% of herniated discs migrated to the near-upward position, of the superior, while 3.5% of the cases moved to the far up-ward position. In the two cases reported here, inadvertent intradiscal injection may have occurred due to an intervertebral disc herniation (protruding) into the superior foramen in the path where the block needle was advancing. The post-operative MRI in case 2 confirmed a right superior foraminal disc herniation. However, in case 1, the MRI was performed at another hospital before the operation, and the images could not be confirmed. Therefore, for patients with herniated discs, adjustments of the needle's location must be made according to the location and extent of the herniated discs using MRI, if possible.
For the infrapedicular approach reported by Begduk et al. [9], to place the needle at the anterior epidural space, the needle is directed toward a target point on the upper margin of an imaginary triangle (the "safety triangle"), formed by a base tangential to the pedicle, a line tangential to the lateral margin of the vertebral body, and the hypotenuse coincident with the upper margin of the spinal nerve and the dorsal root ganglia; then the needle is advanced in the 6-o'clock position to the pedicle and the advancement is made using lateral fluoroscopy. However, Lee et al. [2] reported that the posterolateral technique, which places the needle in a more posterior position, had similar effects and Goodman et al. [10] suggested the retroneural approach, which places the block needle in the posterior position. The lateral margin of the safety triangle was suggested to be an ideal point, by Pfirrmann et al. [11]. The retrodiscal approach, in which the needle is advanced past the target point of the lateral margin of the superior articular process, was reported by Jasper et al. [12] to provide reliable contrast imaging. Such variation in the procedures used for the TFEI suggest that the optimal tip of the block needle may vary among reported patients, considering the extent of anatomical deformities, pain during the procedure, and the clinician's preferences. Further studies are needed to compare the methods used and the patient outcomes to determine the optimal approach.
In cases where TFEI is scheduled for patients with a herniated disc suspected based on symptoms and physical examination only, positioning the tip of the needle as far as to the superior epidural space would be expected to reduce the frequency of intradiscal injections. In previous case reports, then the needle was drawn back, after discogram confirmation, and the contrast medium was injected again, satisfactory contrast patterns were achieved [3,5]; while the MRI imaging in those cases confirmed a herniation of the intervertebral disc that changed its position from the anterior foramen space. Based on such evidence, when a block needle is advanced to the posterior surface of an expected foramen, under lateral flu oroscopy, the frequency of complications can be reduced by confirming the images with contrast medium before the advancement of the needle, and by a careful placement of the needle by assessing the resistance with its advancement. In cases where correction of the placement of the block need le is required, a small amount of contrast medium or contrast diluted with saline should be used to prevent the injected contrast medium from blocking the fluoroscopic view.
The frequency of discitis, after a block needle is advanced into intervertebral discs, is not known. In cases with a discogram, however, the frequency of discitis has been reported to range from 0% to 4.92% of patients and 0% to 3% of discs injected [13]. When discogram is performed, it needs more rigid sterile manipulation with using intravenous or intradiscal antibiotics [13,14]. Therefore, the possibility of the incidence of discitis should not be overlooked when a block needle is advanced into the disc during the TFEI. There was a case report that they experienced intervertebral injection during the TFEI, but that not considering it as a complication but applying medication both to the nerve root area and disc, good results were obtained [10]. However, discitis may develop after an epidural injection with the transforaminal approach [15]; in addition, resistance to antibiotics or severe neurological complications associated with discitis may occur. Therefore, the preventive use of antibiotics is recommended [3].
In conclusion, the TFEI requires a well-prepared pre-operative study on the anatomical configuration and a careful decision on the placement of a block needle in consideration of the irritated nerve. It also necessitates considering the preventive use of antibiotics against additional infections in case of intradiscal injection.







 XML Download
XML Download