

 PDF
PDF Citation
Citation Print
Print


Introduction
Cancer is the leading cause of death in Korea. Over 200,000 new cancer cases are diagnosed annually, and 1 in 4 deaths is caused by cancer [1].
Population-based cancer survival estimates reflect the average prognosis for a given cancer type, as they are based on unselected patients with a variety of natural histories as well as treatment patterns. Although the cancer stage at diagnosis is the most important prognostic factor for patients' survival, there are limited population-based studies of stage-specific survival, especially those in Asian countries [2,3].
The Korea Central Cancer Registry (KCCR) has published national cancer statistics annually, including incidence, mortality, survival, and prevalence, since 2009 [4]. From the data on incidence in 2003, the KCCR collected information regarding the stage at diagnosis using the Surveillance, Epidemiology, and End Results (SEER) summary stage. Summary staging is a basic way of categorizing how far a cancer has spread from its origin. Several cancer registries in the North America report their data by the summary stage, as the staging categories are broad enough to measure the success of cancer control efforts and other epidemiologic efforts [5]. The KCCR has reported the disease stage distribution of incident cases from 2005 to 2010 [6], and it is possible to calculate survival by the stage at diagnosis using this data.
This study aimed at reporting the stage-specific survival rates for the 8 most common cancers diagnosed during the period 2006-2010 in Korea and at comparing the stage-specific survival rates between Korea and the US.
Materials and Methods
The Korean Ministry of Health and Welfare started a nationwide, hospital-based cancer registry called the KCCR in 1980. Details of the history, objectives, and activities of the KCCR have been documented [7]. The primary cancer was classified according to the International Classification of Diseases for Oncology 3rd edition [8] and converted to the classification system used by the International Classification of Diseases 10th edition [9]. The analysis was restricted to the most frequent 8 cancer sites and to patients aged≥20 years, because childhood cancers differ from adult cancers in many respects. Cases of cancer at the following 8 sites were analyzed: stomach (C16), colorectum (C18-C20), liver (C22), lung (C33-C34), female breast (C50), cervix uteri (C53), prostate (C61), and thyroid (C73). Records were excluded if the diagnosis was established by death certificate only and in cases where the year of birth or death was not known. The survival analysis used 626,506 cancer cases for the selected cancer sites diagnosed during 2006-2010, for whom the vital status of patients was followed up until December 31, 2011. Passive follow-up was conducted using mortality database maintained from the Statistics Korea and population registration database from the Ministry of Security and Public Administration. The duration of survival for each case was determined as the duration from the date of initial diagnosis to the date of death, loss to follow-up, or date of follow-up termination, whichever came first.
Age at diagnosis was classified into 4 groups: 20-49, 50-64, 65-74, and ≥75 years. Stage at diagnosis was classified as localized (invasive cancer confined to the organ of origin), regional (spread to adjacent organs and/or regional lymph nodes by direct extension), distant (extension to organs other than those covered in the regional category or metastases to distant organs or distant lymph nodes), or unknown. The KCCR records constituted the best available information on the stage of disease as it appears in the medical record within 4 months of diagnosis.
Relative survival is a net survival measure representing cancer survival and the absence of other causes of death. Relative survival rates (RSRs) were defined as the ratio of the observed survival rate to the expected rate; this was based on a group of people in the general population similar to the patient group with respect to sex, age, and calendar period of observation [10]. Therefore, the survival experience of the patients was adjusted for the average life expectancy of the general population of the same age, which makes the RSR an estimate of the chance of surviving the effects of cancer. Additionally, a RSR of 100% implies that a cancer patient cohort is just as likely to survive the given interval as a cohort in the general population of the same sex and age; it does not mean that everyone in the group has survived cancer.
The RSRs were calculated using the Ederer II method [11]. Relative survival analyses were based on an algorithm developed in SAS by Paul Dickman, with some minor adaptations. Asymmetric observed survival confidence intervals (CIs) were formed from standard errors estimated using Greenwood's method [12] and log (-log) transformation. All analyses were conducted using SAS version 9.2 (SAS Institute Inc., Cary, NC).
Results
Table 1 shows the basic characteristics of 626,506 cancer patients with the 8 cancer types selected for this study that were diagnosed in 2006-2010. Cancers of the stomach, colon and rectum, liver, and lung were found to be more frequent in men than in women, whereas higher proportion of thyroid cancer was observed in women (84.2% of thyroid cancers reported). The median age at cancer diagnosis was the oldest in prostate cancer cases (70 years) and the youngest in cases of female breast cancer (49 years). With respect to the stage at diagnosis, the percentage of localized cancer varied from 18.3% to 56.4% by the cancer site. Of the 8 cancer types examined, lung cancer was the most severe with 40.6% of cases defined as distant, compared to only 1% of thyroid cancers. SEER stage was unknown in 9.9-20.2%, which varies by cancer types.
Table 2 shows the 5-year RSRs and 95% CIs for the 8 cancer types by sex, age group, and stage at diagnosis. The overall 5-year RSR was the highest for thyroid cancer (99.8%) and the lowest for lung cancer (19.7%). The 5-year RSRs for stomach, colorectal, liver, and thyroid cancers were similar or higher in men (67.7%, 74.5%, 26.6%, and 99.8%, respectively) compared with women (65.7%, 69.9%, 26.7%, and 99.7%, respectively), whereas those for lung cancer were much higher in women (25.4%) than in men (17.5%).
For most cancer sites, the 5-year survival rates in younger individuals were higher than that for individuals aged ≥75 years. Indeed, the 5-year RSRs for patients aged ≥75 years were lower than that for all other age groups.
There was considerable variation in the distribution of the stage at diagnosis. For stomach, colorectal, female breast, cervix uteri, prostate, and thyroid cancers, the 5-year RSRs for localized stage disease were >90%. Conversely, the 5-year RSRs for liver and lung cancers were 42.8% and 46.3%, respectively. Survival rates for patients with distant stage cancers ranged from 2.5% to 69.1%, with patients with liver cancer showing the lowest and those with thyroid cancer showing the highest RSR. For all 8 cancer sites, the 5-year RSRs for patients with unknown stage at diagnosis were lower than that of the overall RSRs.
Table 3 shows the stage distribution and 5-year RSRs for 5 cancer sites by sex. For stomach, colorectal, and liver cancers, the stage distribution in men and women were similar and survival rates were similar for every stage at diagnosis. In cases of lung cancer, women had a higher proportion of distant stage lung cancer than men, whereas the survival rate for distant stage lung cancer was much higher in women. Among patients with distant stage thyroid cancer, men had poorer stage-specific survival than women.
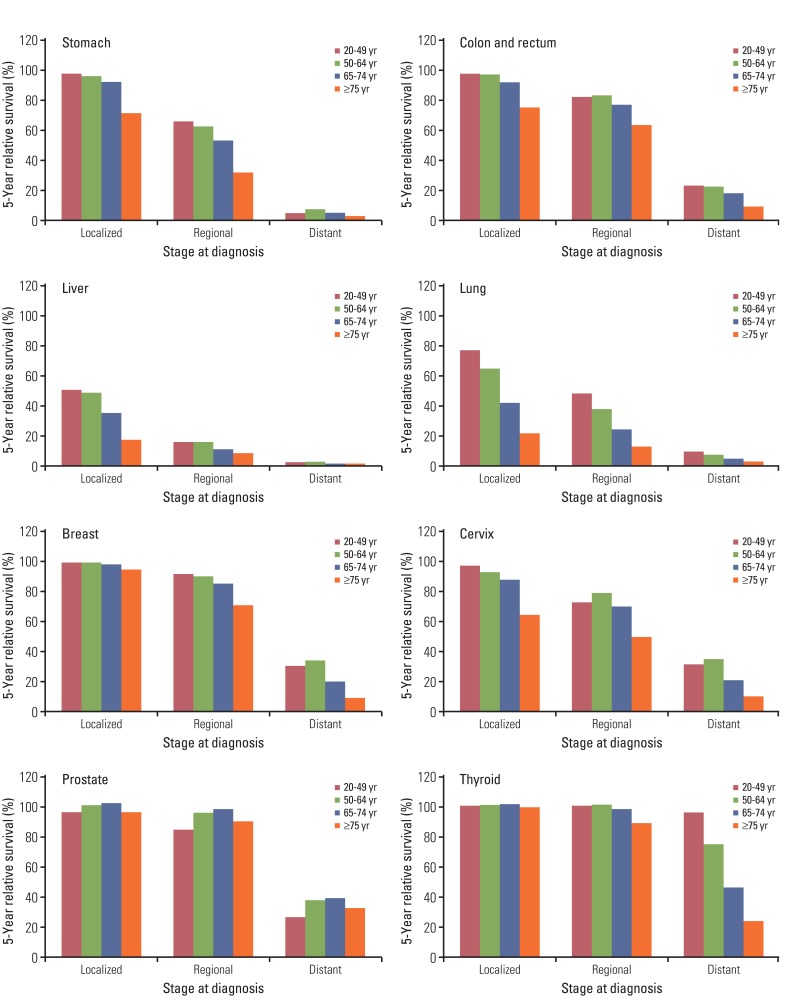
Table 4 and Fig. 1 present the distribution of stage at diagnosis by age group and the 5-year RSRs for the 8 cancer sites. Diagnosis with localized stage cancer of the stomach, colorectum, liver, breast, cervix uteri, and prostate was more common among younger individuals than among older individuals. There was substantial variation by age group and stage at diagnosis. Survival rates for all the selected cancers except for the prostate cancer showed decreasing trends with age across all stages of disease. In general, younger patients showed better survival than older patients, whereas prostate cancer patients aged 20-49 years had worse survival outcomes than patients aged ≥50 years. However, unknown stage for prostate cancer, patients who were aged ≥75 years had worse survival outcomes than patients aged <75 for all stages of disease.
Table 5 shows the comparison of stage distribution and survival rates of cancer patients from Korea and the US. Korean patients with stomach cancer and cervical cancer are more likely to be diagnosed at early stage of disease and were observed better stage-specific survival than among patients from the US. Conversely, for prostate cancer survival, Koreans are less likely than US patients to be diagnosed with early stage.
Discussion
The extent of disease at diagnosis is the most important prognostic factor for patients' survival. The 5-year RSR for each stage at diagnosis, except for stomach and prostate cancer, was much higher in younger than in elderly patients, with the differences being greater for stomach, lung, and cervical cancers. Several studies have reported poor survival and the need for different strategies for elderly cancer patients [13-15]. This may be due to the advanced stage at diagnosis or the presence of comorbidities [15,16], as well as difficulty in accessing care or the lack of availability of appropriate care [17].
The 5-year survival rate for Korean patients with stomach cancer during 2006-2010 was 67.0%, whereas that for American patients during 2002-2008 was 26.9% (Table 5). The prognosis for Korean patients was better mainly because of a more favorable stage distribution than that observed for American patients. Approximately 51% of patients with stomach cancer had localized disease, whereas, tumor spread to distant organs or lymph nodes was identified at the time of diagnosis in 34% of cases in the US. However, only 26% and 12% of stomach cancer cases in Korea were classified as having regional and distant metastasis, respectively. The Korean government initiated a nationwide stomach cancer screening program for men and women aged ≥40 years in 1999, which appears to have led to earlier diagnosis and treatment of stomach cancer. According to a recent report from the Korean Gastric Cancer Association [18], the proportion of patients diagnosed with early-stage gastric cancer has markedly increased from 28.6% in 1995 to 57.7% in 2009. Populations with a higher incidence of stomach cancer have better survival rates than those with a lower incidence [19]. In addition, survival of patients with stomach cancer is partly influenced by the tumor location and histological type. Tumors located in the gastric cardia have a much poorer prognosis than non-cardia gastric cancer. Differences in median age, body mass index, lymph node dissection between Korean and US patients also maybe in part explain the different survival rates of gastric cancer at the same stage [20]. The 5-year survival rate for Korean patients with stomach cancer has dramatically increased from 43.0% and 42.6% for men and women, respectively, diagnosed between 1993 and 1995 to 67.7% and 65.7% for men and women, respectively, diagnosed between 2006 and 2010 [1].
For prostate cancer, the 5-year RSRs were 90.2% and 99.2% in Korea and the US, respectively. Further, 82% of prostate cancer cases in the US were localized compared with only 54% of cases in Korea. Analysis of SEER data indicated that the 5-year RSR for prostate cancer patients in the US increased from 83.2% in 1987-1989 to 99.9% in 2001-2007 [21]. Although this improvement partly reflects the increasing proportion of localized or regional prostate cancers diagnosed, stage-specific increases in survival rates have also been observed. The incidence of prostate cancer in Korea increased by 12.8% annually from 1999 to 2010, and an improvement in survival was observed for patients with prostate cancer (from 55.9% in 1993-1995 to 90.2% in 2006-2010) [1]. The results showed that age-specific five-year relative survival was poorer in the age groups 20-49 and ≥75 years, compared to age groups 50-64 and 65-74. Similar trend was also observed in the US. Some studies exhibited the aggressive biologic behavior and rapidly fatal outcome in younger diagnosed with prostate cancer. It is possible that young prostate cancer patients tend to have more advanced disease and histological grade considered because prostate cancer is very rare prior to age 50 and may be diagnosed as a result of symptomatic disease [22].
Similarly, the 5-year RSR for patients with cervix uteri cancer in Korea (80.2%) was much higher than that for patients in the US (67.9%). Regional stage disease is diagnosed less frequently among Korean than US women (25% vs. 36%) and the stage specific 5-year survival rate for Korean (70.9%) than for US (56.7%). Human papillomavirus is considered a necessary cause of cervical cancer, it has been shown that various lifestyle and behavioral aspects, such as reproductive factors, contraceptive use, and smoking, are related factors for cervical cancer risk. Other most important factor, screening reduces advanced stage detection of cervical cancer. Currently, population-based organized cervical cancer screening programs are implemented free of charge all Korean women aged 30 over biennially [23].
For lung cancer, 41% patients in Korea had distant spread at diagnosis. However, complete diagnostic information required for staging was not available in 16% of cases. The stage distribution in men and women was similar, but survival rates were much higher for women, which may be explained by histological differences between genders. Adenocarcinoma was the most common cancer in women, and survival rates among patients with adenocarcinoma was higher than that among patients with squamous cell carcinoma, which was the most common histologic type in men. Smoking and alcohol consumption are predictors of survival in lung cancer [24]. Further, comorbidities could increase the overall mortality among cancer patients.
Overall, survival rates of patients with breast cancer vary by age at diagnosis. The 5-year RSR was 97.6% for localized cancer, and 89.2% for cancer with regional spread. For women diagnosed with regional spread, those aged ≥75 years had a 5-year RSR of 70.3% compared to 89.1% and 83.9% observed in those aged 50-64 years and 65-74 years, respectively. Differences by age group were even greater for cases of distant metastasis.
The 5-year survival rate for patients with thyroid cancer was greater than 99.8%, and the RSRs of patients aged <75 years with localized thyroid cancer or those aged <65 years with regional spread cancer was over 100%. The relative survival estimate of greater than 100% for Korean patients diagnosed with localized thyroid cancers indicates that the observed survival of these cancer patients was actually higher than that of the general population. There are at least 2 possible explanation for this result: it could reflect a selection bias with a higher proportion of people screened from a higher socio-economic group with a lower mortality risk [25], or a diagnosis of thyroid cancer could increase the likelihood that patients undergo medical interventions, which may have a positive impact on their general health and overall survival.
The results of this study should be interpreted with caution. First, the validity of the survival estimates depends on the completeness of cancer registration. In particular, selective under-estimates of patients with a poor prognosis may lead to over-estimation of cancer patient survival. However, the completeness of cancer registration in Korea was reported to be over 97% [1], which is relatively good. Second, validation of stage information is critical for comparing survival rates. Many registries have routinely collected stage-at-diagnosis data using the SEER summary due to the ease of data collection from medical records. Although the SEER stages are not as detailed as those defined by other staging systems, reports indicate that the SEER stage provides an effective adjustment for stage at diagnosis. However, the proportion of unknown stage cases reported in Korea was relatively high, which makes it difficult to compare the survival rate by stage distribution directly for some cancer sites. Third, we used all subjects who are diagnosed from 2006 to 2010 as incident cancers until the closing date of the follow-up in the analysis. This approach is widely practiced in survival analysis by cancer registry. In this approach, those under observation for a variable period of time and having an incomplete follow-up of less than five years are included, apart from the subjects with a complete follow-up of five years. This approach may lead to under-estimation compared to survival under the condition of full follow-up, because survival expectation of newly diagnosed cancer patients will be higher in the case of recent improvement in prognosis.
Conclusion
This study provides the first population-based stage-specific survival analysis for 8 major cancers in Korean adults. Korean cancer patients showed relatively favorable stage distribution and 5-year RSRs, which suggests potential contribution of the national cancer screening program. This information will be useful for clinicians and cancer patients, as well as for policy makers evaluating and planning the national cancer control program.
 XML Download
XML Download