

 PDF
PDF Citation
Citation Print
Print


Introduction
Colorectal cancer is one of the most common cancers in the Western countries. In Korea, colorectal cancer is the second most frequently diagnosed cancer and its incidence is increasing (1). A number of recent studies have analyzed the clinical and biochemical aspects of colon cancers based on their location, i.e., right-sided, left-sided or rectal (2-5). However, more than 80% of left colon cancers occur in the sigmoid colon. Less common are the cancers occurring between the distal transverse and descending colon, which are termed splenic flexure (SF) cancers.
Therefore, the clinicopathologic characteristics of SF cancers are poorly defined, and the optimal surgical treatment for SF cancer remains to be established. Some surgeons believe it is best to manage such cancers with extensive surgery, such as an extended right hemicolectomy or combined splenectomy (6,7).
The present study sought to identify the clinicopathologic characteristics of these infrequent SF cancers and to compare them with the features of right-sided colon and left-sided colon cancers (with excluding the SF cancers). This study also compared the outcomes and complications of the surgical procedures used to treat the near SF cancers in order to identify the optimal procedure.
Materials and Methods
We reviewed the medical records and the colorectal cancer database of 3,964 colorectal cancer patients who underwent surgery at our clinic between June 1993 and June 2003. The study only included the patients who had main tumors located the SF and that were histologically proven adenocarcinomas, and there were 167 of these patients (4.2% of all the colorectal cancer patients).
The SF was defined as being from the distal third of the transverse colon to the descending colon, with excluding the sigmoid-descending junction. Colon obstruction was classified into either 1) acute complete colon obstruction, which was defined as radiographic signs of abdominal distension and abnormal gaseous distension of the bowel with laparotomy findings of proximal bowel distension and edema, and urgent surgery was performed within 48 hours of admission (8), or 2) partial colon obstruction where intestinal continuity was maintained, but the obstruction could not be traversed with a flexible 13.2 mm external diameter colonofiberscope.
The patients underwent either a left hemicolectomy (LHC) or subtotal colectomy. LHC was performed by carefully mobilizing the SF and its mesentery, and then dividing the left colic artery and the left branch of the middle colic artery at their origins, removing the entire lymph-node-bearing mesentery and sampling the inferior mesentery lymph nodes. Bowel resection involved half of the transverse colon proximally and the proximal sigmoid colon distally to the extent of securing an adequate distal resection margin. Bowel anastomosis was performed as end-to-side or side-to-end with using a circular stapling device.
The American Joint Committee on Cancer (AJCC) 6th edition classification and stage groupings were used for tumor assessment. The patients were followed-up postoperatively every 6 months for the first 2 years and then annually thereafter until death or until they were lost to follow-up. The evaluations included clinical examinations, common blood chemistry tests, assessing the serum CEA level, chest radiography and abdominal and pelvic CT. Colonoscopy was performed annually and those patients with suspected recurrence or metastases underwent specific examinations (e.g., CT, MRI and bone scans). Recurrence was confirmed radiologically or by biopsy. The median follow-up period was 82 months (range: 1~184 months).
Of the 156 patients who underwent surgery with a curative intent, adjuvant chemotherapy was administered postoperatively to 136 patients (87%). A floropyrimidine-based regimen was used for adjuvant chemotherapy: 5-FU/leucovorin were given to 109 patients (70%), oral floropyrimidine was given to 25 patients (16%) and FOLFIRI (5-FU/leukovorin/irinotecan) was given to 2 patients (1%).
Of the 167 patients, 114 (68.3%) were alive at the time of this investigation (August, 2008). Recurrence of colorectal cancer followed by death occurred in 37 patients (22.2%), while 16 patients (9.6%) died of other causes with no evidence of colorectal cancer recurrence. There were no death-related, immediate postoperative complications (within 1 month of surgery).
The study also involved 200 consecutive patients out of the 798 patients with right-sided colon cancer and 200 patients out of the 900 patients with sigmoid-descending junction & sigmoid (SD & S) colon cancer. The right-sided colon was defined as the portion that included from the cecum to the proximal two-thirds of the transverse colon, while the left-sided colon, except the SF, was the SD & S colon.
The categorized data were analyzed using chi-square tests, and the continuous variables were compared using independent sample t-tests. The patients who underwent palliative resection were not included in the survival analysis. The overall survival (OS) and disease-free survival (DFS) were compared using the Kaplan-Meier method. The risk factors associated with overall survival were compared using the Kaplan-Meier method, and the potential variables were verified by multivariate analysis using a Cox regression model. All the tests were two-tailed, and a p value less than 0.05 was considered to indicate a significant difference. All the statistical calculations were performed using SPSS software (ver. 12, SPSS Inc, Chicago, IL).
Results
The 167 SF cancer patients were comprised of 113 men and 54 women, and the mean age was 55 years (range: 14~85 years). The most common clinical manifestation was abdominal pain (59.3%). Resection with a curative and non-curative intent was performed in 156 (93.4%) and 11 (6.6%) patients, respectively. Fourteen patients (8.4%) had complete colon obstruction and 118 patients (70.7%) had partial colon obstruction.
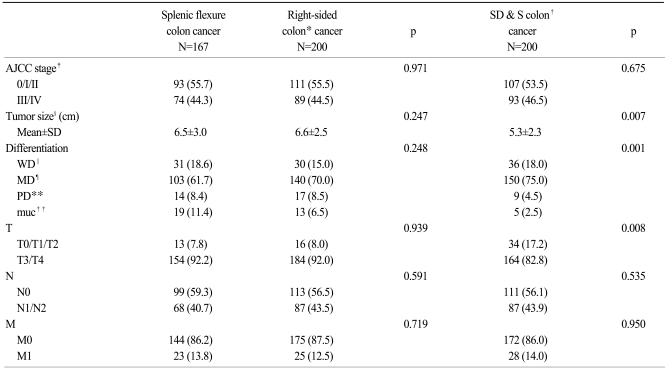
The mean longest diameter of the tumors was 6.5±3 cm (range: 1~19). According to the cell differentiation, 103 patients (61.7%) had moderately differentiated cancer, 31 patients (18.6%) had well-differentiated cancer and 14 patients (8.4%) had poorly differentiated cancer. In addition, 19 (11.4%) patients had mucinous adenocarcinomas. A summary of the clinical and pathological features of the near SF cancer patients is shown in Table 1 and 2.
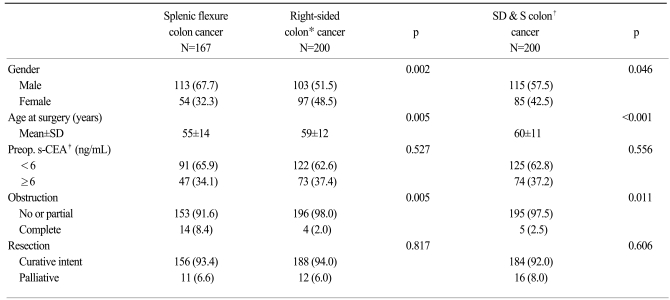
1. Comparison of the clinicopathological characteristics and survival for the patients with splenic flexure, right-sided colon and SD & S colon cancer
The clinicopathologic characteristics of the patients with SF, right-sided colon, and SD & S colon cancers were compared. All three cancer types were found to be similar in terms of the preoperative CEA level, operative curability, T factors, N factors and M factors. However, the cancers differed in terms of the gender ratio, age, obstruction, the maximal tumor diameter and the histologic type (Table 1 and 2). Compared to the right-sided colon or the SD & S colon cancers, the SF cancers were more common in males, the cancers were diagnosed at a younger age, the cancers were more commonly obstructing and they were more commonly mucinous adenocarcinomas. The SF cancer tumors were similar in size to the right-sided colon cancers, but the SF cancers were larger than the SD & S colon cancers.
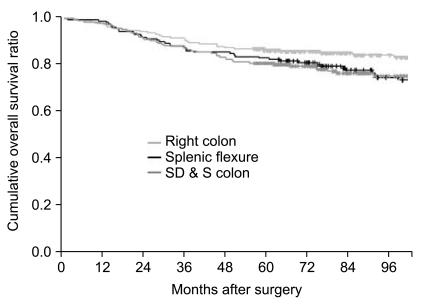
There were no significant differences in the survival rates between the patients with SF, right-sided colon and SD & S colon cancer and who underwent surgery with a curative intent (Fig. 1).
2. Effect of combined spleen resection
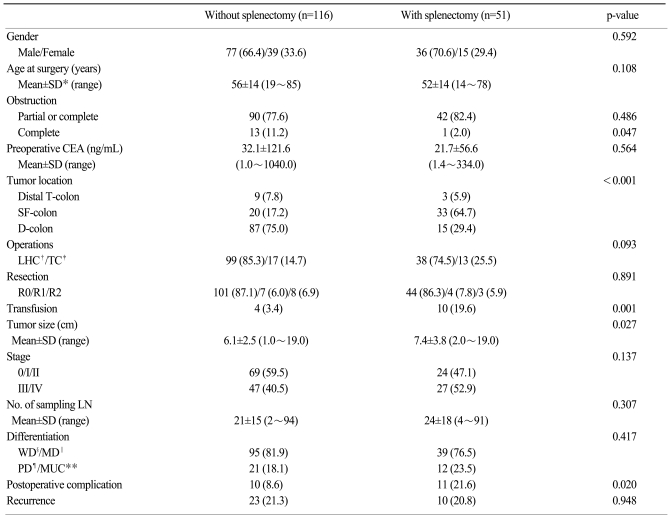
Of the 167 SF cancer patients, 51 (30.5%) underwent a colectomy and a combined splenectomy. Combined splenectomies were performed because of the tumor proximity to the spleen (≤2 cm) in 35 (68.6%) cases, and extended surgery was performed due to possibly advanced tumor in eight (15.7%) cases, bleeding in five (9.8%) cases and for other reasons (previous total gastrectomy in two and tumor thrombus in the splenic vein in one) in three (5.9%) cases.
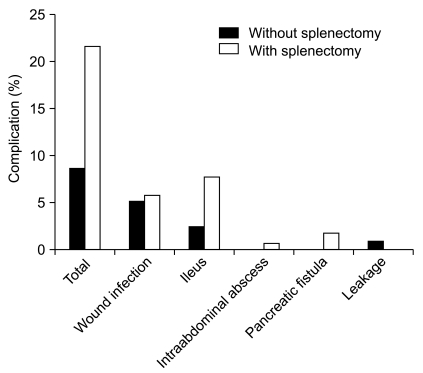
Tumors were frequently located at the SF in the splenectomy group. The mean longest diameter of the tumors was larger in the splenectomy group as compared to the no splenectomy group (7.4±3.8 vs. 6.1±2.5 cm, respectively, p=0.027). The frequency of transfusions during surgery was higher in the splenectomy group as compared to the no splenectomy group [10 (19.6%) vs. 4 (3.4%) patients, respectively, p=0.001]. Postoperative complications were more frequent in the splenectomy group as compared with the no splenectomy group [11 (21.6%) vs. 10 patients (8.6%), respectively, p=0.02] (Table 3) (Fig. 2).
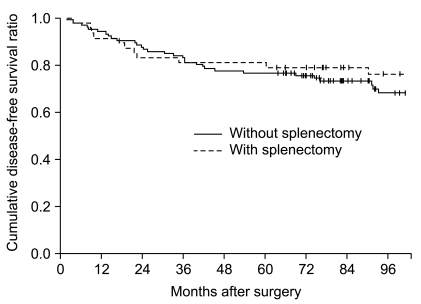
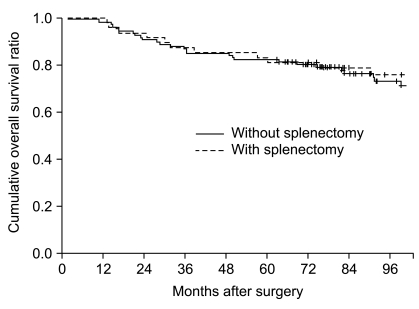
The splenectomy and no splenectomy groups did not differ in terms of mean overall survival (138.1±9.5 vs. 129.5±7.3 months, respectively, p=0.297) or disease-free survival (144.3±8.5 vs. 137.6± 6.9 months, respectively, p=0.395) (Fig. 3, 4)
Lymph node metastasis developed in 68 (40.7%) of the 167 patients. Lymph node metastasis, other than pericolic and intermediate metastasis, was identified in four cases, namely, two patients with metastasis along the splenic hilum, one patient with metastases along the principal lymph nodes at the left colic artery and one other patient with metastases along the lymph nodes at the inferior mesentery vein.
3. Comparison of left hemicolectomy vs. subtotal colectomy
Of the 167 near SF cancer patients, 30 (18.0%) underwent a subtotal colectomy, and these were due to synchronous cancer in seven cases, multiple polyps in five cases, obstruction in five cases, a family history in five cases, metachronous cancer in four cases and extended surgery in four cases. Compared to the patients who underwent a LHC, the subtotal colectomy patients had more sampled lymph nodes (19±13 vs. 33±24, respectively, p<0.001), a higher intra-operative transfusion rate (7 (5.1%) vs. 7 (23.3%) patients, respectively, p=0.001) and a higher postoperative complication rate (14 (10.2%) vs. 7 (23.3%) patients, respectively, p=0.05). Of all the subtotal colectomy patients, only one showed lymph node metastasis along the right-side colic vessel, while all the others showed regional lymph node metastases adjacent to their tumors.
The LHC and subtotal colectomy groups did not differ in terms of mean overall survival (143.6±6.0 vs. 121.8±10.9 months, respectively, p=0.439) or disease-free survival (135.3±6.4 vs. 117.0±12.3 months, respectively, p=0.656).
4. The recurrence pattern and the risk factors for survival
Recurrence developed in 54 patients following curative resection for SF colon cancer, and this was comprised of hematogenous metastasis in 25 patients, seeding in 16 patients, lymph node metastasis in seven patients, metachronous cancer in five patients and local recurrence in one patient.
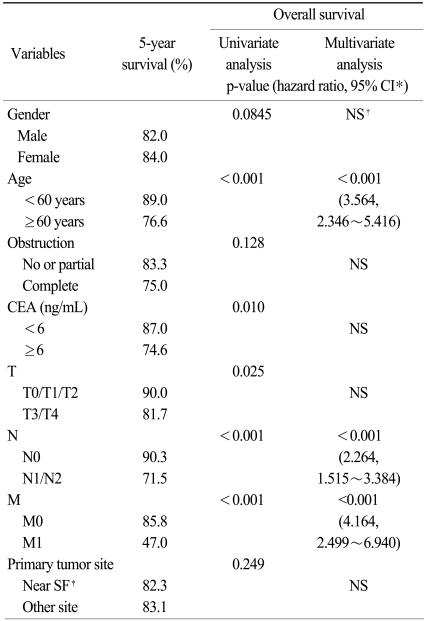
Cox' proportional hazards model was used to identify the independent risk factors for overall survival after surgery. For the patients who underwent curative intent surgery, eight variables were included in the analysis. Multivariate analysis showed that an older age (≥60 years), the N factor and the M factor were the independent risk factors for overall survival (Table 4).
Discussion
The SF colon cancers are known to be relatively rare, and these account for 2~5% of all the colorectal cancer occurrences (6,7,9,10). The present study found that 4.2% of all colorectal cancer patients had tumors located in the SF, and that 17% of the left-sided colon cancer patients had tumors at this site. Therefore, most left-sided colon cancers originated from the sigmoid colon and their characteristics had the possibility to differ from those of SF cancers.
We found that SF cancers were more predominant in males, as compared to right-sided colon or SD & S colon cancers. In addition, the SF cancer patients were younger than the patients with right colon or SD & S colon cancers. A previous study reported that the patient age did not differ among the different cancer sites, and that left colon cancer occurred more commonly in males than did the cancers that occurred at other sites (8). Other studies found that left-sided colon cancers were more common in younger people and in males as compared to the right-sided cancers (2,5).
SF colon cancers carry a high risk of obstruction. Some studies have reported that the incidence of obstruction for these cancers is approximately four times that of other colon cancer sites (8), and others have reported that the risk of obstruction is almost 50% (6). The present study also showed a high frequency of obstruction for the SF colon cancers (8.4% were completely obstructed). This high frequency may reflect that the SF has an acute angle, and that the SF tumors tended to be relatively large. The diameter of the SF tumors was similar to that of the right colon cancers, and the diameter of the SF tumors was larger than that of the left colon cancers. However, since the diameter of the right-sided colon was larger than the left-sided colon, obstruction frequently occurred for patients with the SF cancer. CT colonography may be helpful to evaluate the proximal colon for such a condition.
The incidence rate for mucinous adenocarcinoma has been reported to be 10~20% in Western populations and 4~7% in Asian populations (11,12). In general, mucinous cancers are more prevalent in the right-sided colon and rectum and they are larger tumors than the non-mucinous cancers (12). Our previous study found that the incidence of mucinous adenocarcinoma was 7.5% of the right-sided colon cancers and 4.3% of the left-sided colon cancers (12). The present study found that the incidence of mucinous cancer was high (11.4%) for the SF colon cancers. This may correlate with the SF colon cancers being larger than the sigmoid colon cancers. Further studies are warranted to investigate a possible pathogenic link between SF colon cancers and mucinous cancers.
The embryonic midgut develops into the right-sided colon, which extends from the cecum to the proximal two-thirds of the transverse colon. The right-sided colon is vascularized by the superior mesenteric artery. In contrast, the embryonic hindgut develops into the left-sided colon, which extends from the distal third of the transverse colon to the upper anal canal; this is vascularized by the inferior mesenteric artery (5). The goal of surgical treatment for resectable carcinoma of the colon is to remove the tumor with an adequate margin by performing a wide excision of the tumor-bearing area and the associated lymphatics (10). However, the blood supply to the SF has been shown to be variable in that the blood supply is carried by the inferior mesenteric artery via the left colic artery in 89% of the cases and by the superior mesenteric artery via the middle colic artery in 11% of the cases (13). Therefore, a carcinoma at this site has dual lymphatic drainage: to the superior mesenteric vessel via the middle colic vessel, and to the inferior mesenteric vessels via the left colic vessel. In addition, the SF has direct lymphatic drainage to the splenic hilum and along the pancreas tail (9). For this reason, some surgeons recommend extended colectomy, including splenectomy, for treating SF cancer. While some authors recommend routine splenectomy and distal pancreatectomy (6), others found that such procedures did not improve 5-year survival of SF cancer patients (14). Khafagy et al. (14) reported direct pathologic invasion of the spleen in 10% of the cases of SF cancer that received colectomy with splenectomy. We found that there was no direct invasion of the spleen for the 51 cases with combined splenectomy, and that only one case showed splenic metastasis due to tumor emboli of the splenic vessels.
The previous studies have reported no lymph node metastasis at the splenic hilum in the patients with SF cancer and who underwent combined splenectomy (9,14-16). In the current series, there appeared to be two cases of splenic hilar lymph node metastasis. In one case, the patient had tumor emboli in the splenic vein, and the tumor recurred in the liver and pancreas at nine months after surgery; the patient died 24 months after surgery. In the other case, one of nine lymph node metastases was a splenic hilar lymph node metastasis, and there was no evidence of disease at 113 months of follow-up. We found that splenic hilum lymph node metastasis was very rare in patients with SF cancer. Therefore, selective splenic hilum lymph node sampling was required in only limited cases of primary advanced cancer with suspected hilum lymph node metastasis. Imaging studies such as positron emission tomography (PET) may be helpful for making the diagnosis of splenic hilum lymph node metastasis.
Some surgeons recommend subtotal colectomy or extended right hemicolectomy to achieve a better oncologic outcome for SF cancer patients (6,17). In contrast, other investigators (7) reported that because SF cancers do not carry a worse prognosis than colon cancers at other sites, the dual lymphatic drainage did not confer a survival disadvantage and extended resection was unnecessary. Sadler et al. (17) reported on lymph node metastasis at the ileocolic junction in a patient who underwent an extended right hemicolectomy. Other studies reported no lymph node metastasis at the root of the middle colic artery in six patients (9). In our study, one of the 30 total colectomy patients showed lymph node metastasis along the right-side colic vessel. That case had already shown lymph node metastasis along the origin of the superior mesenteric artery, and the patient died at 21 months after surgery.
Some studies have reported that an incidental splenectomy contributed to the morbidity and mortality of the primary operation, and that these patients had a higher transfusion requirement (18-20). We found that the rates of postoperative complications and transfusion were higher in the combined splenectomy group and subtotal colectomy group as compared to the LHC group. Most of the studies that have examined the effect of splenectomy on the long-term survival of colorectal cancer patients have reported that splenectomy did not influence long-term survival (20-22). However, Davis et al. (23) demonstrated no difference of survival in patients with Dukes B cancer according to splenectomy, but the Dukes C patients who underwent splenectomy had significantly poorer outcomes. Despite an assumption that a splenectomy may affect survival due to the oncological or immunological effects, we found that there was no difference in disease-free survival or overall survival between the splenectomy and non-splenectomy patients in this study. In addition, the disease-free survival and overall survival were similar for the subtotal colectomy and LHC patients.
Our multivariate analysis showed that old age (≥60 years), being node positive and a M1 status were the independent factors affecting overall survival, and this was regardless of the cancer site, the same as was reported elsewhere (24,25). Colonic obstruction in large bowel cancer is generally considered a poor prognostic factor. However, our multivariate analysis showed that complete colon obstruction did not affect survival, and this is consistent with a previous study (8). This probably reflects that there was no perforation with obstruction in the patients with left colon cancers, and so there was no immediate postoperative mortality.
Conclusion
The infrequent SF colon cancers exhibited different characteristics such as a male predominance, the patients were diagnosed at a younger age and a high incidence of mucinous adenocarcinoma and obstruction as compared to the patients with colon cancer at other sites. There was no difference in surgical outcomes between the patients who underwent an LHC as compared to those who underwent extended surgery (i.e., combined splenectomy or subtotal colectomy). Therefore, LHC appears to be sufficient for a satisfactory oncologic outcome, and this indicates that performing a concurrent splenectomy is generally unnecessary for the patients with SF colon cancer.
 XML Download
XML Download