

 PDF
PDF Citation
Citation Print
Print


Introduction
Multiple primary cancers refer to the condition where more than two cancers occur independently in an individual. There have been many reports about multiple primary cancers since Billroth first reported on it in 1889 (1) and then Warren and Gates summarized it in 1932 (2). Multiple primary cancers make up 3~7% of all the cases of cancer. The wide range of the incidence reflects the lack of consistent definitions and the selection of patient groups (3). Among many cancers, bladder cancer has the highest incidence rate among the urologic cancers (4). Yet penile carcinoma is an uncommon condition, and this accounts for less than 1% of all male cancers in the United States and 0.04 per 100,000 in Korea (5,6). Penile cancer is even more uncommon when it is combined with other cancers. We describe here an extremely rare case of synchronous double primary cancer involving the bladder and penis.
Go to : 
Case Report
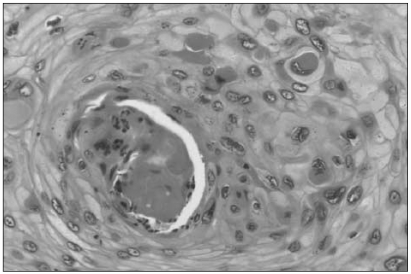
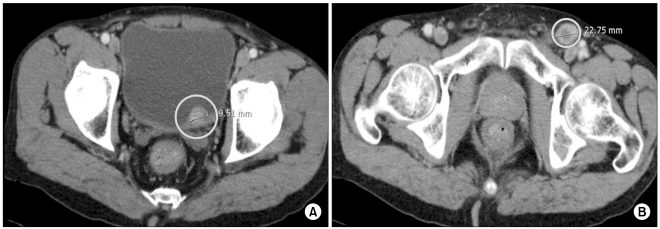
A 64-year-old man was referred from a primary urological clinic and he presented with a painful penile mass. The mass was located on the upper right dorsal side of the penis, and it measured approximately 2.5 × 2 cm in size. Upon physical examination, there was no other palpable mass in the inguinal and abdomen areas. We performed a biopsy of the penile mass and the histology revealed a well-differentiated squamous cell carcinoma (Fig. 1). The bone scan was normal and a computed tomography (CT) scan of the abdomen and pelvis showed a localized bladder tumor and one enlarged lymph node in the left inguinal area. The bladder tumor on the left posterior wall was 1 cm in size and it was a localized, enhanced, protruding polypoid mass (Fig. 2A). There was a 2.2 cm sized lymph node in the left inguinal area, and it had an enhancing peripheral portion on the post contrast enhancement scan phase (Fig. 2B). We checked the routine laboratory data, and it was all within the normal range.
The patient underwent a partial penectomy, transurethral resection of the bladder tumor (TURB) and an inguinal lymph node dissection. The pathology results from the TURB revealed a high-grade papillary carcinoma, which had invaded the subepithelial connective tissue, with a tumor-free resection margin (Fig. 3A). Among the five dissected inguinal lymph nodes, a single lymph node that was 1.2 cm in size showed metastatic squamous cell carcinoma (Fig. 3B). The TNM stage of the penile and bladder tumor was T1N1M0 and T1N0M0, respectively. The final diagnosis was double primary cancer of the penis and bladder.
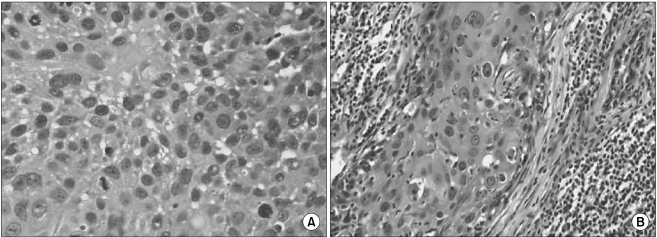 | Fig. 3(A) The pathologic features of the bladder tumor (H&E stain, ×200). The microphotograph showed an invasive urothelial carcinoma with more nuclear pleomorphism, anaplasia and many mitotic figures. (B) The pathologic features of the left inguinal lymph node (H&E stain, ×100). The microphotograph showed a metastatic squamous cell carcinoma with less differentiation and more nuclear pleomorphism and mitotic activity.
|
After two months of the recovery period, the patient received adjuvant radiotheraphy and systemic chemotherapy to treat the penile cancer. The external radiotherapy was done with the 2-dimensional conventional irradiation method and using a 15 MV photon beam. The primary tumor site of the penile cancer and the adjacent tissues were treated with 54 Gy in 30 fractions per 6 weeks. Simultaneously, according to the result of a favorable response to the current chemoradiotherapy, cisplatin (90 mg/m2) was administered on day 1 and fluorouracil (5-FU) (1,300 mg/m2) was administered from days 1 to 4. The chemotherapy was done every 3 weeks for 4 cycles. During a total of 12 weeks of the chemotherapy, there was no complication except for mild nausea.
The follow-up CT scan of the abdomen and pelvis and the positron emission tomography (PET) that both were done six months after the operation showed no evidence of recurrence.
Go to :
Discussion
Multiple primary cancers are defined as two or more cancers that do not have any subordinate relationship and the cancers develop independently. The diagnostic criteria for multiple primary cancers that were advocated by Warren and Gates in 1932 are summarized as follows (2). First, each cancer must be definitively malignant according to the histopathology. Second, they must be histologically different. Third, the possibility of metastasis among the cancers must be excluded. The occurrence of multiple primary cancers has increased since Billroth first reported a case of tumors in multiple organs. This increased occurance is a result not only of the population aging, but it is also caused by the advances in medical technology, and particularly those of the diagnostic techniques and cancer treatment modalities. The cure rates and survival rates have also increased for the same reasons (7). The incidence of multiple primary cancers in Korea, including double primary cancer, was reported to be 0.35% in 1970 and 1.43% in 1999 (8,9).
Bladder cancer has the highest incidence rate of all the urologic cancers. The crude incidence rate of bladder cancer is 4.43 and 0.98 per 100,000 in males and females, respectively (4). Penile cancer rarely occurs in the developed countries. For example, the incidence rate of penile cancer was 0.58 cases per 100,000 persons in the United States between 1993 and 2002 (5) and 0.04 cases per 100,000 persons in Korea between 1998 and 2002 (6). To the best of our knowledge, only one case of synchronous multiple primary cancers, including penile cancer and hepatocelluar carcinoma, has been reported by Kang et al. in Korea (10).
Moertel et al. classified the multiple primary cancers observed at the same time or within six months as synchronous multiple primary cancers, and cancers developing with more than a six month interval as metachronous multiple primary cancers (11). Our case is an example of the synchronous type. The mechanism of multiple primary cancers is not fully known, but many hypotheses have been suggested, such as a family history, immunologic and genetic defects, prolonged exposure to carcinogens, the radiation and chemotherapy administered for the primary cancer and field cancerization (12). Thus, multiple primary cancers have been investigated with the goal of examining the environmental and host factors that increase the risk of cancer and for identifying the adverse consequences of cancer treatment. In this present case, the etiologies of the bladder and penile cancer were different. The possible etiologies of penile cancer include human papilloma virus infection, phimosis, poor hygiene and cigarette smoking (13). The possible etiologies of bladder cancer include schistosomiasis, chemical exposure, pelvic radiotherapy and smoking (14). However, the patient in this case was a non-smoker.
There are no established therapeutic rules for multiple primary cancers, but the type, progression, response to therapy and the patient's general health status should be considered. If each of the cancers has the possibility to be cured, then radical therapy is indicated. If radical therapy of the primary cancer is impossible, then conservative therapy is indicated for the secondary cancer. However, the management of penile cancer is still controversial. Treatment of the primary penile tumor tends to be more organ-preserving in order to maintain sexual function and a better quality of life. The organ-preserving treatment is generally the most favorable; patients with penile carcinomas and a favorable histology (stages Tis, Ta, T1; grades 1 and 2) are at a low risk for local progression and distant metastatic spread (15). However, in this case, we chose partial penectomy with a lymph node dissection, and then adjuvant radiotherapy and chemotherapy, including cisplatin and 5-FU, for achieving a cure.
Multiple primary cancers have rarely been reported in Korea, but it is believed that the incidence is rising. Prevention, making an early diagnosis and the treatment of multiple cancers will become even more important in the future.
Go to :
 XML Download
XML Download