

 PDF
PDF Citation
Citation Print
Print


Introduction
The alkylating agent ifosfamide is an anti-neoplastic used in both pediatric and adult age groups to treat various malignancies. Although its potential for urologic toxicity is tempered by mesna (sodium 2-mercaptoethane sulphonate) pretreatment, glomerulopathy, tubulopathy, and hemorrhagic cystitis still occur as adverse events in a considerable number of patients (1,2). Fanconi's syndrome, a proximal tubulopathy marked by excessive urinary excretion of glucose, phosphate, bicarbonate, amino acid and protein, is likewise a noted complication, with rickets and growth retardation as long-term consequences. Adults are rarely affected, but this syndrome is not infrequent in children as a clinical expression of ifosfamide-induced nephrotoxicity (3,4). Several published reports have also linked a combination of ifosfamide and cisplatin to persistent renal function decline requiring hemodialysis (5). We report here a 67-year-old patient who received a regimen of ifosfamide, adriamycin and mesna for epithelioid sarcoma and soon thereafter developed a proximal renal tubulopathy, in conjunction with hemorrhagic cystitis. To our knowledge, this is the first documented instance where Fanconi's syndrome (nephrotoxicity) and hemorrhagic cystitis (urotoxicity) jointly resulted from one-time ifosfamide exposure, without contributory cisplatin.
Go to : 
Case Report
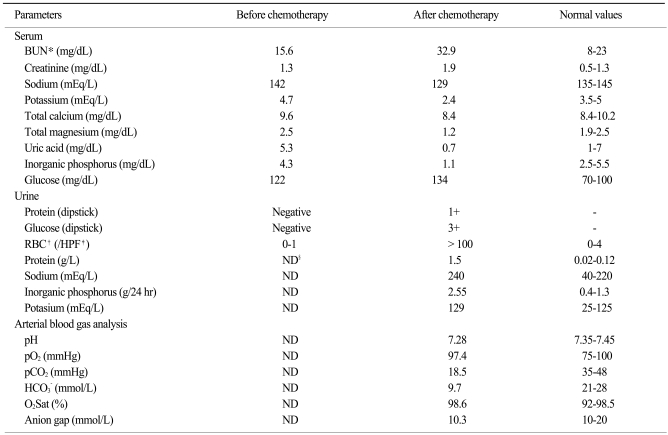
The patient, a 67-year-old male, presented at our clinic with dysuria and gross hematuria. He had a 6-month history of type 2 diabetes mellitus, treated with an oral hypoglycemic agent. More recently, a malignancy was discovered when he sought treatment (debridement) for an inflamed right fifth toe. Following amputation of the right fourth and fifth toes and right inguinal lymphadenectomy, a histologic diagnosis of epithelioid sarcoma was rendered. Following pretreatment with mesna (4,350 mg/m2), he subsequently received one course of adriamycin plus ifosfamide (5 g/m2 for one day). Laboratory values at baseline included a serum creatinine of 1.3 mg/dL and a glomerular filtration rate of 51.5 mL/min/1.73 m2. His urine had tested negative for both protein and occult blood, with a specific gravity of 1.1.
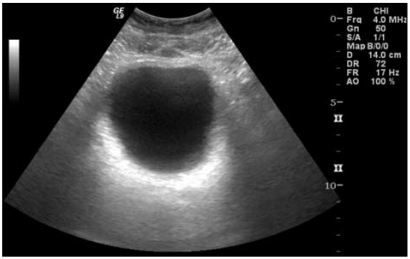
Seven days after chemotherapy, the patient was admitted with a blood pressure of 130/80 mmHg, a pulse rate of 80/min, a respiratory rate of 20/min and a body temperature of 36.3℃. Percussion at the costovertebral angle was pain-free, but palpation of the abdomen elicited mild tenderness. The complete blood count showed white blood cells (WBC) at 310/mm3; lymphocytes, 220/mm3; monocytes, 40/mm3; neutrophils, 40/mm3; eosinophils, 10/mm3; hemoglobin, 13.1 g/dL; and hematocrit, 50,000/mm3. A serum profile revealed a creatinine of 1.9 mg/dL; sodium 129 mEq/L; potassium 2.4 mEq/L; inorganic phosphorus 1.1 mg/dL; total magnesium 1.2 mg/dL; and uric acid 0.7 mg/dL. Urinalysis displayed 1+ protein, 3+ glucose, and red blood cells >100/HPF. As measured by 24-hour urine, total protein was 1.5 g; inorganic phosphorus 2.55 g; and potassium 129 mEq/L. Arterial blood registered a pH of 7.28; HCO3 9.7 mmol/L; and anion gap, 10.3 mmol/L (Table 1). The size and shadow of both kidneys were normal by ultrasound, and a diffuse thickening of the bladder wall was noted (Fig. 1).
By the second hospital day, the patient was febrile (39℃). Antibiotics and granulocyte-colony stimulating factor (G-CSF) were initiated, and he was given supportive fluid therapy. Bladder irrigation was also scheduled, but was discontinued after one attempt due to severe pain and discomfort. Most of the patient's symptoms subsided by day 6 of hospitalization, when he was afebrile with a normal neutrophil count, and the gross hematuria had resolved. His urine samples were microscopically devoid of organisms, and cultures of the urine and blood (each in triplicate) were consistently negative. Without laboratory evidence of acute cystitis or pyelonephritis (i.e., negative urinary nitrite and normalized WBC/CRP), piperacillin/tazobactam antibiotic coverage was stopped. He was discharged from the hospital after 14 days, having fully recovered.
The patient is seen periodically in follow-up at our outpatient clinic. Urinalysis and a 24-hour urine test were unremarkable seven days postdischarge, but his serum creatinine had climbed to 1.5 mg/dL. A score of 8 by Naranjo adverse drug reaction probability scale indicated a strong likelihood that the proximal renal tubular dysfunction experienced in this setting was linked to ifosfamide therapy. Further adjuvant chemotherapy with the ifosfamide/adriamycin regimen was thus declined.
Go to :
Discussion
Risk factors for the nephrotoxicity of ifosfamide include cumulative dosing, unilateral nephrectomy, and concomitant use of cisplatin (1-3). Some studies, conducted with children or relative youths, have also proposed that the associated risk may be age-dependent (1). The applicability to adults is therefore questioned. Our patient, while diabetic, was treatment naïve with respect to cancer therapy and was not otherwise at risk as currently defined. He nonetheless developed a proximal tubulopathy and hemorrhagic cystitis (gross hematuria and lower abdominal pain) seven days following a single course of ifosfamide-containing chemotherapy, but finally recovered after two weeks of conservative treatment. This certainly upholds the concept that ifosfamide may prove nephrotoxic in the absence of reported risk factors.
The spectrum of ifosfamide nephrotoxicity is broad, ranging from asymptomatic tubulopathy to overtly impaired renal function or outright renal failure, and has been well documented (4). Even after discontinuation of this drug, the tubulopathy may progress to end-stage disease, so that hemodialysis is sometimes required. Our patient displayed features typical of Fanconi's syndrome; hypophosphatemia, hypokalemia, hypouricemia, proteinuria and glucosuria. Although beta-2 microglobin and amino acids were not monitored, the 24-hour urine results confirmed a proteinuria of 1.5 g/day and high phosphorus output, together suggesting proximal tubular damage.
The mechanism of ifosfamide nephrotoxicity has been attributed to the metabolites 4-hydroxyl ifosfamide, chloracetaldehyde and acrolein. Chloracetaldehyde, especially, suppresses activation of complex-I (NADH-ubiquinone oxidoreductase) in the mitochondrial respiratory chain, resulting in decreased intracellular glutathione and ATP and inhibiting Ca2+ signaling, thus inducing cell death. The cellular impact of chloracetaldehyde, and hence the threat of nephrotoxicity, cannot be averted with preventative use of mesna (5).
Hemorrhagic cystitis is a fairly regular accompanimont of ifosfamide, manifested by dysuria, suprapubic discomfort, and gross or microscopic hematuria. Although this complication is often circumvented with mesna, it still occurs in a considerable number of patients (6). The ifosfamide metabolite, acrolein, is subject to renal excretion. It augments the production of nitric oxide synthase in urothelium and generates various cytokines (TNF-α and IL-1β) through intracellular transcription modulation to increase reactive oxygen species and nitric oxide levels. Hemorrhagic cystitis thereby results, variably involving mucosal edema, hemorrhage, necrosis and ulceration.
The sulfhydryl radical of mesna combats ifosfamide urotoxicity by combining with and eliminating acrolein (1). Proper hydration, of course, is required; but the fact that mesna prophylaxis does not uniformly prevent hemorrhagic cystitis in ifosfamide recipients implies that direct urothelial insult by acrolein may not be the sole pathogenic determinant. Perhaps cytokines such as TNF-α and IL-1β and their roles in nitric oxide production provide an over-riding mechanism for the urotoxicity of this drug (7).
This patient fortunately recovered with just two weeks of conservative treatment. However, at follow-up, his serum creatinine level had edged up to 1.5 mg/dL, and the nephropathy of diabetes was implicated. Because his renal status may continue to deteriorate, he is monitored periodically, with strict attention to blood glucose control. It is consequently our view that diabetic nephropathy, in addition to age as a risk factor, may trigger adult susceptibility to ifosfamide nephrotoxicity. Further studies will be needed to confirm such speculation.
Go to :
 XML Download
XML Download