

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
A recent major breakthrough in medical oncology has been the demonstration of efficacy in randomized phase III clinical trials of antiangiogenic drugs, in particular bevacizumab (Avastin®), the 'targeted' anti-VEGF monoclonal antibody, when combined with standard chemotherapy. Such trials have shown clinical benefit (in progression free survival or overall survival) in advanced colorectal cancer, advanced non small cell lung cancer, as well as for response rate and progression free survival in metastatic breast cancer (1). How a "tumor starving" drug such as bevacizumab enhances the efficacy of conventional chemotherapy remains something of a mystery although there are a number of different theories currently being studied (1,2). Also interesting is that chemotherapy itself may have effects on tumor angiogenesis (3,4) either by targeting dividing endothelial cells present in the tumor's growing neovasculature (a local antiangiogenic effect), or by mobilizing bone marrow derived proangiogenic cells such as circulating endothelial progenitor cells (CEPs) - a systemic and potentially proangiogenic effect (3). However, it appears that an overall significant antiangiogenic effect is obtained when chemotherapy is administered in a so-called "metronomic" fashion (3), the extent of which can be amplified by concurrent combination with an antiangiogenic drug such as VEGF or VEGF receptor targeting antibodies.
METRONOMIC CHEMOTHERAPY
Metronomic chemotherapy refers to the close, regular administration of a chemotherapeutic drug at relatively low (non-toxic) doses, over prolonged periods, with no extended drug-free break periods (5). As such it can be viewed as a form of "dose dense" chemotherapy but differs from most forms of the latter in several ways (3). First, it is not necessarily "dose intense" where the goal remains to deliver greater cumulative levels of drug, at shortened intervals, e.g. once every two weeks instead of once every three weeks. Second, because metronomic regimens are much less toxic, they do not usually require hematopoietic growth factor support (e.g. using recombinant G-CSF), or other supportive care measures (6,7). Metronomic chemotherapy can thus be viewed as a form of long term 'maintenance' chemotherapy that can be used on its own (3,5), or perhaps more importantly, combined over long periods of time with biologic targeted therapies, especially antiangiogenic drugs such as anti-VEGFR-2 antibodies (8) or small molecule multi-targeted VEGFR-2 antagonist receptor tyrosine kinase inhibitors (9) and possibly other drugs or therapies such as trastuzumab (Herceptin®) (10), tumor vaccines (11), or even aromatase inhibitors such as letrozole (12). It can also be integrated and sequenced with standard MTD type chemotherapy where brief courses of such induction therapy, given 'upfront', is followed by long term maintenance/metronomic low-dose chemotherapy (sometimes called "chemo-switching") (9) combined with a concurrent targeted therapy (8,9). Among the advantages of metronomic chemotherapy include reduced acute toxicities such as high grade myelosuppression, vomiting, nausea, mucositis, etc. (6,7), sometimes surprisingly good anti-tumor activity (based mostly on preclinical studies so far), even when used to treat drug resistant tumors (5), reduced costs when using off patent chemotherapeutic drugs (13), and increased convenience when using oral drugs which can be taken at home (3,6). These potential advantages could be useful for long term adjuvant therapy of early stage cancers. Long term daily oral administration of a drug such as UFT (an oral 5-FU prodrug) for 2 years with no breaks might be viewed as an example, in retrospect, of metronomic chemotherapy (14). This current major disadvantage of translating metronomic chemotherapy into the clinic is the empiricism associated with determining the optimal biologic dose (OBD).
CHEMOTHERAPY CAN AFFECT TUMOR ANGIOGENESIS, BOTH NEGATIVELY AND POSITIVELY
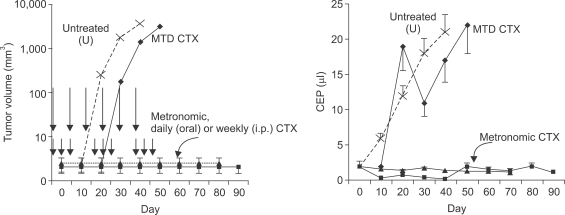
There is growing interest in the idea that chemotherapy drugs can inhibit tumor angiogenesis, and that this 'side effect' of chemotherapy may contribute to its anti-tumor activity, in addition to direct cytotoxic effects on tumor cells. The basis for the hypothesis that chemotherapy can target tumor angiogenesis originally stemmed from the observation that a hallmark of angiogenesis is the presence of dividing endothelial cells in sprouting blood vessel capillaries (15,16). Such cells should be sensitive to most chemotherapy drugs which are designed to preferentially target cycling cells (4,17). Indeed there is evidence that most known chemotherapy drugs can suppress angiogenesis using a variety of commonly used in vivo assays (4). Indeed if a chemotherapy drug such as cyclophosphamide is given in cycles of maximum tolerated dose (MTD) therapy separated by long drug -free intervals (to allow recovery from some of the toxic effects of such therapy such as myelosuppression) to tumor-bearing mice, there is evidence of rapidly-induced endothelial cell apoptosis in the tumor's vasculature. But this does not necessarily lead to the expected antiangiogenic effect. The reason is that this damage to the tumor endothelium can be largely and rapidly reversed during the extended drug free break periods (5), perhaps by a massive hemopoiesis-like mobilization ('rebound') of circulating endothelial progenitor cells (CEPs) from the bone marrow (18) (Fig. 1) which could conceivably then home to the damaged tumor endothelium and set about repairing the damage (CEPs are discussed in more detail in the next section). Thus shortening the break periods is critical to ensuring the repair process is prevented or minimized (5). This in turn requires relatively low doses of drug to be used for each drug treatment (5). These results may also help explain why, in some cases, an antiangiogenic drug such as bevacizumab increases the efficacy of standard maximum tolerated dose chemotherapy: the acute systemic CEP rebound occurring during the break periods, which is also observed clinically (19), would presumably be suppressed or blocked, thus preventing a potential 'reactive' pro-tumor angiogenic response (2). Another mechanism, put forward by Hudis (20) is that the local tumor cell repopulation/rebound that occurs after MTD chemotherapy would be presumably slowed by the presence of an antiangiogenic agent, since repopulating tumor cells would require optimal oxygen and nutrients supplied by the tumor vasculature for optimal (re)growth. Thus blocking angiogenesis would be expected to increase progression free and/or overall survival times in such circumstances. In summary, MTD chemotherapy can have an initial local (i.e., intra-tumoral) antiangiogenic effect but this is quickly followed by a reactive and potentially proangiogenic (CEP) systemic effect which may negate the initial antiangiogenic local effect. However, the latter proangiogenic effect can be blocked by use of an antiangiogenic drug such as bevacizumab along with MTD chemotherapy; overall maximal and sustained inhibition of tumor angiogenesis can be achieved by using metronomic chemotherapy regimens combined with a targeted antiangiogenic drug.
IMPACT OF ENDOTHELIAL PROGENITOR CELLS
The aforementioned results highlight the possible impact that bone marrow-derived circulating progenitor cells might have a significant impact on response to chemotherapy and/or antiangiogenic drugs. As such the concept of CEPs deserve special mention.
Until 1997, it was generally accepted that all new endothelial cells in a sprouting (angiogenic) vessel capillary were derived from the division of pre-existing differentiated endothelial cells. However, Isner and colleagues that year reported results showing that up to 20% of the endothelial cells in such vessels were derived from circulating bone marrow cells (21). The methodology used to arrive at such a startling figure was the use of lethally irradiated mice transplanted with syngeneic bone marrow cells which expressed a marker that could distinguish between host and donor bone marrow cell populations, e.g. β-galactosidase (lacZ). A similar methodology has been employed using bone marrow cells transfected with the gene encoding green fluorescent protein (GFP). Such bone marrow chimeric mice are then used as recipients for a tumor transplant, and the tumor associated blood vessels of such tumors carefully examined for the presence of the donor bone marrow derived cell populations within the tumor vasculature using appropriate microscopy techniques which, if properly done, can be used to detect luminally incorporated endothelial cells (derived from the donor bone marrow population). Over the ensuing 10 years many studies have been published utilizing these and similar techniques; the results of such studies have been quite variable in terms of the percentages of bone marrow derived cells incorporated into the lumens of growing tumor-associated blood vessels (22,23). Most studies show much lower percentages than originally reported by Isner and colleagues (e.g. 1~5%) although there are some conspicuous exceptions (where the numbers can be even higher, e.g. 50%) (24,25). This has raised doubts about the impact and relevance of CEPs to tumor angiogenesis (22,23). However, all these studies involved analysis of untreated tumors. As discussed above, the situation might change suddenly and dramatically after therapeutic intervention using certain drugs such as MTD cyclophosphamide which have the ability to cause an acute and massive mobilization of bone marrow derived endothelial progenitor cells, as reported previously (18) and illustrated in Fig. 1.
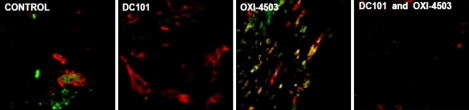
We hypothesized that such acutely mobilized CEPs might subsequently home to drug treated tumors in large numbers and then facilitate tumor repopulation, primarily by amplifying tumor angiogenesis. Indeed, evidence consistent with this hypothesis was reported using a type of vascular targeting drug known as VDAs - "vascular disrupting agents" (26). These drugs, which are mostly microtubule inhibitors, can cause an acute drop in tumor blood flow subsequent to targeting and destroying the established tumor vasculature and thus causing massive intra-tumoral hypoxia and tumor cell necrosis (27). However, a viable rim of tumor tissue almost always remains following VDA therapy from which rapid tumor regrowth ensues. We recently reported a massive invasion and colonization of tumors by bone marrow derived CEPs is induced by VDA therapy (Fig. 2). These cells colonize the viable tumor rim remaining after VDA therapy and moreover contribute to regrowth of the tumors (26), a process that can be blocked by combination treatment using an antiangiogenic drug, e.g. a VEGFR-2 neutralizing monoclonal antibody (DC101), along with the VDA (Fig. 2). More recently, we have observed similar results using a variety of chemotherapy drugs, i.e., acute induction of CEPs which home to the chemotherapy drug treated tumors within a matter of hours to days after a single injection of certain chemotherapy drugs (Shaked et al., unpublished observation). These studies were undertaken after another series of experiments were completed that were designed to determine whether CEPs could be used as a surrogate biomarker for angiogenesis and hence antiangiogenic drug therapy. This was indeed found to be the case based on both pharmacologic and genetic experiments (26). Thus we were able to show that measurement of CEPs in the peripheral blood of mice could help determine the OBD range for targeted biologic antiangiogenic drugs such as DC101 (22).
THE NEED FOR BIOMARKERS TO DETERMINE THE OPTIMAL BIOLOGIC DOSE FOR METRONOMIC CHEMOTHERAPY
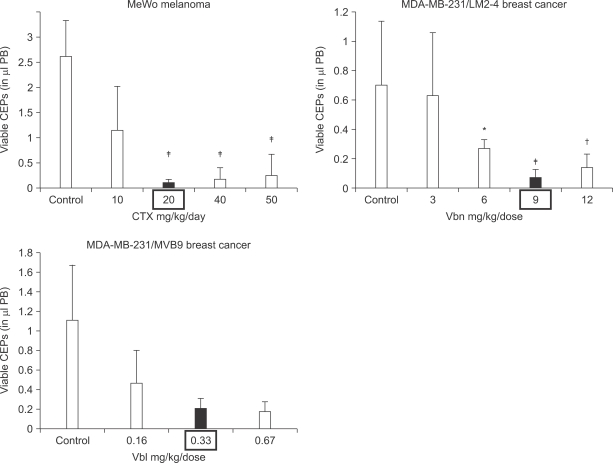
With respect to clinical application, there is at least one significant disadvantage to metronomic chemotherapy as mentioned above: the empiricism associated with determining the optimal 'low' dose, i.e., the optimal biologic (therapeutic) dose (OBD). Because the predominant mechanism for metronomic chemotherapy is thought to be antiangiogenesis (3,5,8) (although other additional mechanisms may be involved as well, such stimulation of the host immune system (28), as a result of targeting both dividing endothelial cells in the tumor's growing vasculature (5) and CEPs (18), we investigated whether these cells could be used as a surrogate marker in mice for determining the OBD for various metronomic chemotherapy regimens (29). The results, an example of which is shown in Fig. 3, showed CEPs can indeed be used successfully for such a purpose in mice (22,29-31). Thus, we can reduce the level of empiricism (at least in mice) when testing metronomic chemotherapy regimens, with respect to determining the OBD.
Whether CEPs can be used as a similarly reliable pharmacodynamic surrogate marker in the clinical setting is problematic given their lower levels in humans compared to mice (23). However, evidence has been obtained recently showing that circulating endothelial cells (CECs) which are apoptotic may be a potentially useful biomarker for metronomic chemotherapy biologic activity (32). Preclinical studies suggest that the likely source of such cells is the tumor vasculature since increases in apoptotic CECs are not detected when normal mice are treated with metronomic chemotherapy (32). However, there is no evidence to show that such cells can be used to help establish the OBD for metronomic chemotherapy in mice or human.
TREATMENT OF ADVANCED HIGH VOLUME METASTATIC DISEASE BY METRONOMIC CHEMOTHERAPY
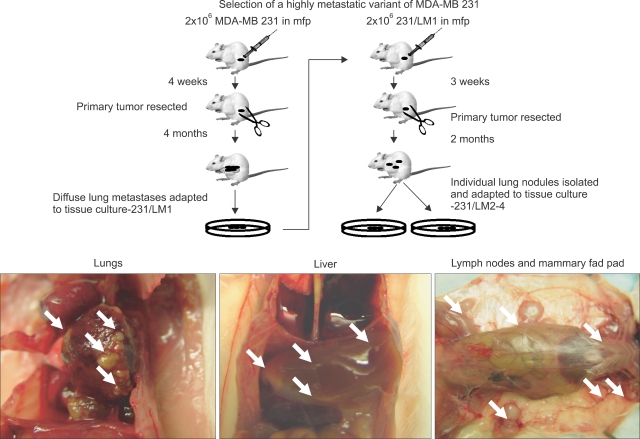
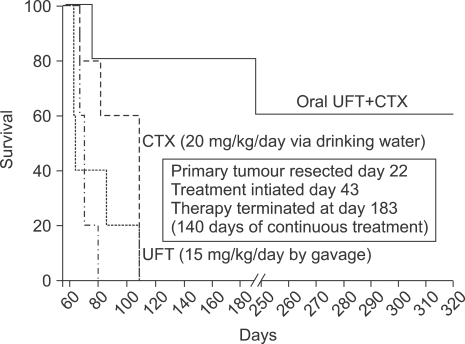
An example of the benefits of reducing the empiricism of metronomic chemotherapy using CEPs to help establish the OBD can be seen from preclinical experiments determining the anti-tumor effects of single versus two chemotherapeutic drug combinations, administered in a metronomic fashion, i.e., daily (by oral delivery) in a model of advanced high volume (end stage) visceral metastatic disease of human breast cancer xenografts where therapy was initiated at terminal stages of disease (31). One drug was cyclophosphamide administered at 20 mg/kg/day - the OBD determined by effects on CEPs, administered through the drinking water (33). The other drug used was UFT administered by gavage every day for 140 days (with or without cyclophosphamide) at the determined OBD, namely, 15 mg/kg (31).
The rationale for undertaking these studies was as follows. First, it is often the case that doublet combinations of chemotherapy, when administering such drugs in an MTD fashion, is superior to mono-chemotherapy in the clinical setting. Second, it is rare for preclinical investigators to undertake studies involving therapy of advanced metastatic disease despite the fact that most phase I and phase II clinical trials involve treatment of such patients. It is well known that it is usually much more difficult to treat advanced metastatic disease, as compared to earlier stage microscopic metastatic disease or primary tumors (34,35). Consequently, this may be a major source for the discrepancy that is often observed between preclinical studies testing various therapies for anti-tumor activity in mice to what is subsequently observed when similar drugs/therapies are tested in cancer patients (34,35). The usual trend is that highly encouraging results in mice are not reproduced in the clinical setting. We reasoned that this discrepancy might be partially resolved by undertaking studies of advanced metastatic cancer in mice and moreover, there might be occasional exceptions to the rule that advanced metastatic disease is much less responsive, or resistant altogether, to a particular anti-cancer therapy. Discovery of such exceptions could be followed by their assessment in the clinical setting, with a great degree of confidence that significant anti-tumor activity might be observed.
With this aforementioned rationale in mind, it was encouraging that we observed truly remarkable long-term survival effects when the combination treatment of metronomic UFT plus metronomic cyclophosphamide was used, in comparison to either drug treatment alone (31) (Fig. 4, 5). The combination of a 5-FU prodrug, e.g. capecitabine and metronomic cyclophosphamide has now advanced to clinical trial testing in the setting of metastatic breast cancer where this combination is being used in combination with bevacizumab in an ongoing phase II clinical trial being undertaken in Milan, Italy at the European Institute of Oncology (36).
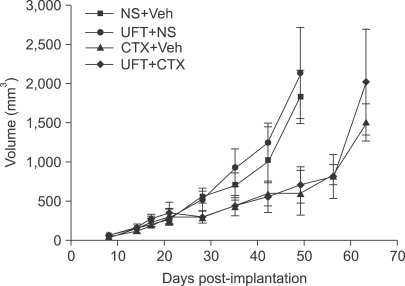
Also of considerable interest with respect to our UFT plus cyclophosphamide preclinical results was the observation that the combination treatment did not have a compelling anti-tumor effect when used to treat primary localized tumors using the same tumor cell lines, transplanted into the mammary fat pad. Indeed the UFT treatment alone did not seem to have any effect in this setting, did not enhance the anti-tumor effect of metronomic cyclophosphamide (Fig. 6). However, subsequent careful analysis revealed that the UFT treatment did have an effect on inhibiting local invasion of the primary tumors as well as inhibiting distant microscopic metastases (31). Thus two important implications emerge from these results. First, lack of response of primary tumors - as measured only by tumor volume changes - may mask other anti-tumor effects that are more subtle, yet biologically important. Second, there may be situations, surprisingly, where high volume metastases may respond better to a particular therapy compared to control primary tumors.
Because of these findings we have embarked on a major program developing models of advanced metastatic cancer in mice, using human tumor cell lines, that are then used for therapy studies.
CLINICAL TRIALS OF METRONOMIC CHEMOTHERAPY
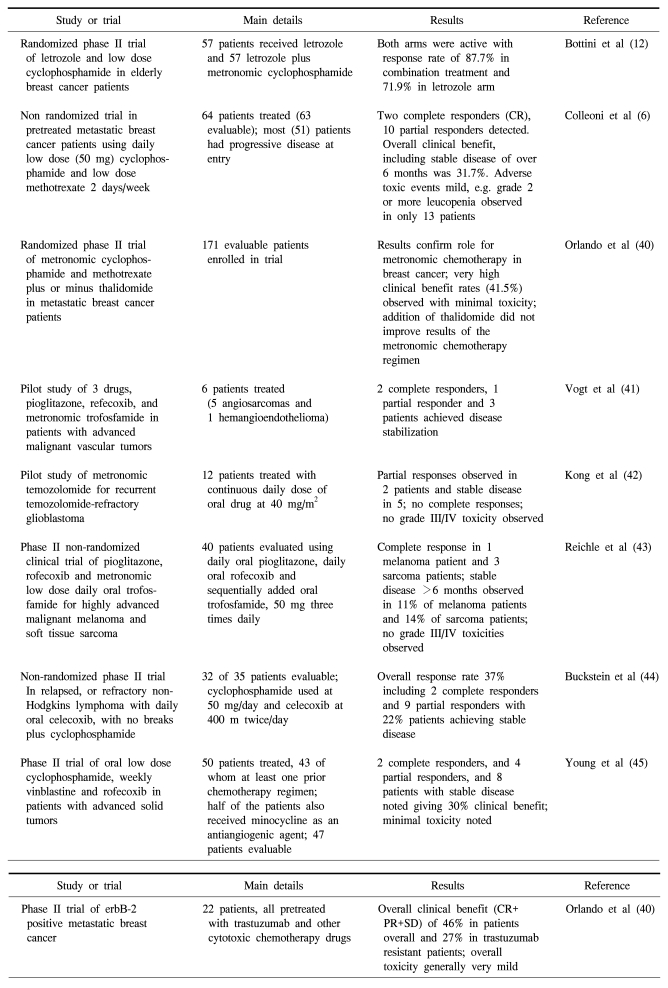
Metronomic chemotherapy regimens have moved into phase II clinical trial testing both in the adjuvant and metastatic settings where they are often combined with a targeted antiangiogenic drug such as bevacizumab (Avastin®), or another targeted agent that likely has some antiangiogenic activity, e.g. the COX-2 inhibitor, celecoxib (Celebrex) (37) or other agents such as letrozole (12) (Table 1). Some interim results of phase II metronomic chemotherapy clinical trials using bevacizumab and daily low dose oral cyclophosphamide in metastatic breast cancer or advanced, recurrent ovarian cancer look extremely promising (38). Ongoing, planned or recently completed (6,39) phase II clinical trials of metronomic chemotherapy, especially those combined with an agent such as bevacizumab should indicate whether or not this treatment strategy has promise in the treatment of metastatic and/or early stage human cancer.
 XML Download
XML Download