

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
In spite of gastric cancer's decreasing incidence and mortality rates, it is still the most common cancer in Korea with the incidence rates being 58.6 and 30.8 per 100,000 for males and females, respectively, during 1999~2001 (1). The ageadjusted mortality rates per 100,000 have decreased from 29.7 in 1983 to 24.3 in 2003 (2), however, gastric cancer still contributes to the large number of cancer-related deaths. Interestingly, there is a trend for the decreasing disease incidence and death in the middle-aged group, but not in the older group (3), and this might be attributed to the rapid changes in life-style and especially dietary habits that have paralleled with the country's economic growth.
In the present study, we examine the temporal trends of gastric cancer mortality in Korea during the past 20 years and we determine to what extent different factors (age, period and birth cohort) have contributed to the trends. Moreover, we predict the gastric cancer mortality in Korea by the year of 2013. Accurate knowledge about the patterns of gastric cancer and its likely evolution in the future will be useful for both planning and organizing prevention, diagnosis and treatment of gastric cancer in Korea.
Go to : 
MATERIALS AND METHODS
The data on the annual number of cancer deaths and the population statistics from 1984 to 2003 were obtained from the Korean National Statistical Office (2). Using this original data, the age-specific gastric cancer mortality rates according to gender were calculated in 5-year age groups (i.e., 25~29 years old, 30~34 years old, ...75~79 years old and over 80 years old) for 5 year periods of time (i.e., 1984~1988, 1989~1993, 1994~1998 and 1999~2003) (Table 1). The birth cohorts were defined by age and the calendar period classifications.
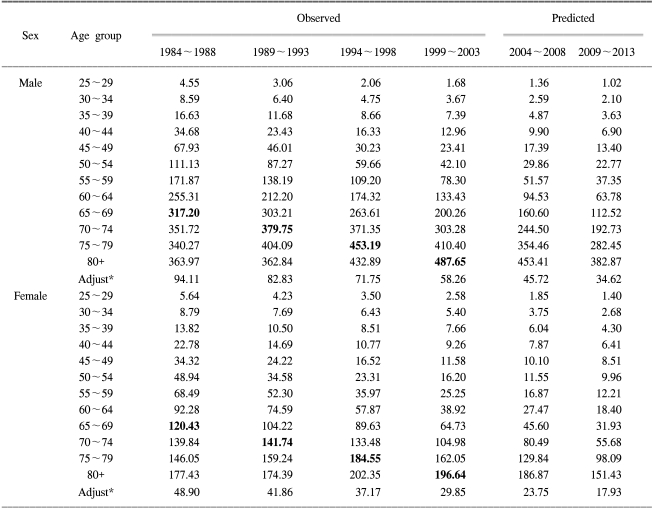
The age adjusted mortality rates were calculated using the 2004~2008 population as a standard. The gastric cancer cases were defined as code C16 in accord with the International Classification of Diseases, 10th Revision (ICD-10).
To estimate the effects of age, calendar period, and birth cohort on cancer mortality, we employed log-linear models with Poisson random variates. In these models, it was assumed that each factor has an additive effect on the log rate (λijk);
logλijk=µ+αi+πj+γk+εijk
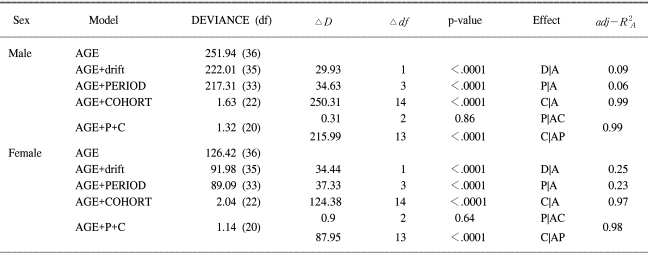
Where, the age effect is represented by αi, the period effects by πj, and the cohort effects by γk. The random error is represented by εijk. The models were fitted using the maximum likelihood method. Based on this general form, we established 5 models in sequence; the one-factor age model first, then the two-factor age-drift model, the age-period model, the age-cohort model and finally the age-period-cohort model (Table 2). The drift term in the age-drift model represents a temporal change in mortality rates that is not identifiable as a period or cohort effect. Goodness of fit was tested and none of the models with more than two factors were rejected (p>0.05). Hence, it was unnecessary to assume there were over-dispersed Poisson random variates in our analysis. The statistical significance of each factor was tested after adjusting for the other factors. Since age is a significant predictor of cancer mortality, goodness of fit with considering age would be valuable. Therefore, age-adjusted R2A was used to evaluate the goodness of fit (4).
To project two periods into the future, i.e., 2004~2008 and 2009~2013, it was necessary to introduce two additional period values and cohort values. The new values were estimated by applying linear regression to the chosen numbers of the most recent period values and cohort values under the assumption that the estimated age, period and birth cohort effect would continue into the future (5). The predicted expected numbers of gastric cancer deaths were calculated using the predicted mortality rates and corresponding populations from the Korean National Statistical Office.
Go to :
RESULTS
Table 1 shows the observed and predicted mortality rates for gastric cancer during 1984~2013 in Korea. For both genders, the observed mortality rates of gastric cancer decreased with the time period for the people with an age under 74, whereas they increased for the people with an age over 74. The observed age-adjusted gastric cancer mortality per 100,000 in men fell from 94.11 to 58.26 during the last 20 years. The predicted expected mortality rates per 100,000 for the males were 45.72 and 34.62 during 2004~2008 and 2009~2013, respectively. The observed age-adjusted cancer mortality per 100,000 for the females fell from 48.90 to 29.85 during the last 20 years. The predicted expected age-adjusted mortality rates per 100,000 for the females are 23.75 and 17.93 during 2004~2008 and 2009~2013, respectively.
Table 2 shows the goodness of fit (scaled deviance) for the age-period-cohort models. Both the period and cohort effect were significant (p<0.001) after adjusting the age effect for the males and females. However, only the cohort effect was significant (p<.0001) when the age-period-cohort model was compared with the age-cohort or age-period sub-model. The values of adj-R2A for the age-cohort model were almost same as those for the full models for both genders. Hence, the age-cohort models were adequate to describe gastric cancer mortality in Korea. There was no reason to apply the full model, which had an unidentifiable problem.
Fig. 1 shows the estimated cohort effects. The risk of gastric cancer death decreased since the 1919 birth cohort for both genders. These decreasing trends were extrapolated into the future for making predictions. The predicted cohort values are marked by open symbols in Fig. 1.
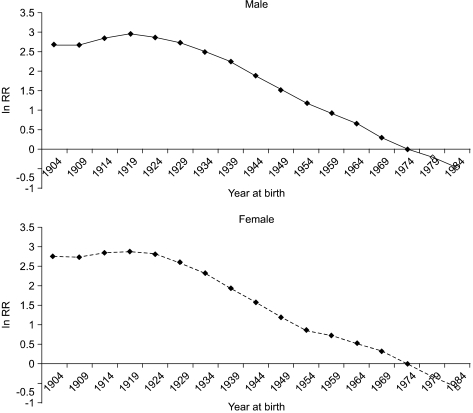
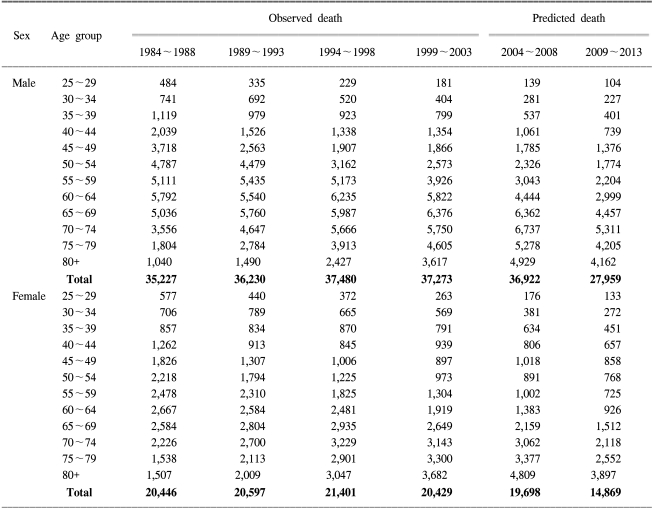
Table 3 shows the observed and the expected number of deaths. During the periods 2004~2008 and 2009~2013, the predicted numbers of deaths due to gastric cancer for males are 36,922 and 27,959, respectively, whereas those for the females are 19,698 and 14,869, respectively.
Go to :
DISCUSSION
This study suggests that age-adjusted gastric cancer mortality in Korea has been decreasing for both genders. The decreasing trend is related with the decreasing risk of cancer mortality since the 1919 birth cohort. The portions of Table 1 corresponding to the 1919 birth cohort are highlighted. Since the 1919 birth cohort has the highest risk for gastric cancer mortality, according to the age-cohort model analysis, the peak of cancer mortality in each age group mainly occurred in the 1919 birth cohort (see Table 1). The age-adjusted mortality rate is expected to steadily decrease in future, and so is the number of gastric cancer deaths.
The declining tendency for the risk of gastric cancer risk since the 1919 birth cohort can be largely explained by the changes of life style, particularly with respect to diet and food storage (6). Since life style is often established in early life, the risk factors closely related with an established life style can be interpreted as cohort factors. Many studies have suggested that consumption of food rich in nitrate, smoked food, a high salt diet and a high starch diet increases the risk of gastric cancer, while consuming large amounts of fresh vegetables, fruits and dairy products is protective against gastric cancer (7). The traditional Korean diet is characterized by a high intake of salty foods and carbohydrates and also a high intake of cooked rather than fresh vegetables. Such Korean foods as broiled meat, i.e., 'bulgogi', thick soybean paste stew, hot pepper-soybean paste stew, soya sauce, picked vegetable, i.e., 'Kimchi', and salted and fermented fish products have been known to increase the risk of gastric cancer (6). In parallel with the economic growth in Korea, the Korean diet has changed to the western style over the past several decades: there is an increased consumption of fresh vegetables, fruit and dairy food such as milk, cheese, yogurt, etc. Unfortunately, the Korean data that directly concerns the change of diet has only existed since the 1980's (8). The Korean intake of fresh vegetable and fruit has increased from 220 g per capita per day in 1976 to 526 g per capita per day in 2003, and the intake of milk has increased from 50.2 g per capita per day in 1985 to 134.86 g per capita per day in 2003 (8). Therefore, the changing dietary habits of Koreans may be protective against gastric cancer (9).
The increase of the use of refrigerators may also play a role to decrease the risk of gastric cancer (10). The nitrates in dried, smoked and salted foods are known to be converted to carcinogenic nitrites by bacteria. The intake of partially decayed foods may introduce potentially dangerous bacteria into the human body. Therefore, the gradual increased use of refrigerators has diminished the ingestion of bacterially contaminated food, and this has reduced the risk of stomach cancer.
Cigarette smoking has been found by several studies to be a risk factor of gastric cancer (3,6). Cigarette consumption in Korea gradually increased by the early 1990's, and then this has remained constant by 2000; however, this has been seen to be recently deceasing (11). However, the change in smoking patterns does not explain the declining gastric cancer risk since the 1919 birth cohort because the decreasing trend in smoking just started recently and gastric cancer deaths have been decreasing since at least the 1980s. Actually, the lung cancer incidence, whose major risk factor is cigarette smoking, is still increasing. Therefore, even if smoking is one of well-known risk factor, its declining trend may not properly explain the decreased gastric cancer mortality. However, it is expected to affect the future trend of gastric cancer.
Another possible reason for the decreasing trend in gastric cancer in Korea might be the decreased exposure to H. pylori infection is recognized as a class I carcinogen for the development of gastric cancer. The organism plays an important role in the pathogenesis of not only persistent gastritis, but also peptic ulcers and gastric cancer (12). The seroprevalence of H. pylori infection in Korean adults has decreased from 80% in the 1980s to the 67% in the 1990s (3). This decreasing prevalence, which is due to a more sanitary environment and the introduction of H. pylori eradication therapy (13), corresponds with the cohort effect.
Even though the trend of gastric cancer mortality in Korea was mainly explained by cohort effect, as is shown in Table 2, there might also be a minor but definite period effect because of the change of classification, improved death certification or the better survival rate. The classification of the gastric cancer did not change during the study period. The proportion of death certificates issued by physicians increased from 44.6% in 1990 to 77.6% in 2002. This improved death certificate generally functions to increase the mortality rate, so it can not explain the decreasing trend of gastric cancer mortality. On the other hand, gastric cancer screening is known to play a central role to reduce this disease's mortality. Note that the 5-year survival rate in Korea is more than 90% for early gastric cancer group, but it's only 20~40% for the advanced cancer group (14,15). One Korean study (16) reported that gastric cancer screening was effective in catching gastric cancer at the early stages, which shows a significant relationship between the timing of gastric examinations and severity of gastric cancer. There are also studies reporting that this screening in Korea has reduced the gastric cancer-related death rate by 48~60% (17,18). Nevertheless, the impact of screening appears to be insignificant in this study period because of the low coverage rate and short history of gastric cancer screening in Korea.
Extrapolation is generally used to predict the incidence and mortality of cancer; this is linear extension of the age-specific rates. However, the cancer mortality at major sites such as the digestive tract, the liver, lung, colon and female breast in Korea is greatly dependent on the birth cohort. Unknown risk factors for cancer may exist and their effect already may be visible for a birth cohort and so improve predictions. In fact, the results of this study are in contrast with those of our previous study that used simple extrapolation (9). On the assessment of future mortality using simple extrapolation, the increase of gastric cancer mortality in the age group over 75 was statistically significant for both genders, and it will contribute to the increasing gastric cancer deaths in the future. If cohort effects are not important, the two prediction methods, i.e., the simple extrapolation and the use of the age-period-cohort model, may give similar estimates of the mortality rates. However, when the cohort effects are significant and the direction of the cohort curve is changed, like that for gastric cancer mortality in Korea, then simple extrapolation fails to recognize the change in direction that's introduced by the cohort effect. Hence, the age-period-cohort model approach may be much more accurate for predicting the future mortality from gastric cancer in Korea.
Any data that would directly show the long-term trend of the gastric cancer incidence rate is not yet available in Korea. Hence, mortality data appears to be the only index of the incidence of gastric cancer. When using this morality data, we should consider the quality of the data in terms of its completeness and validity. The completeness of the data, i.e., the extent to which all cancer deaths that occurred in Korea were included in the database, is know to be reliable since 1980 (19). In terms of validity, the proportion of death certificates issued by physicians was only 77.6% by 2002, and so this may underestimate the true mortality (19). Regardless of the quality of the mortality data, the most notable weak point of performing mortality data analysis for gastric cancer concerns the reduction in case-fatalities by year due to the technologic improvements in screening and treatment. Thus, the simple use of mortality data may overestimate the true decrease (20).
Go to :
CONCLUSIONS
In summary, there was an overall decrease in gastric cancer mortality during 1984~2003 in Korea. The mortality pattern of gastric cancer was dominantly explained by a birth cohort effect, a decrease in exposure to risk factors or an increase in the exposure to protective factors. Therefore, not only the mortality, but also the incidence of gastric cancer in Korea is expected to further decrease in both males and females.
Go to :
 XML Download
XML Download