

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Breast cancer is more frequent in nulliparous women, while its incidence is significantly reduced by a full-term pregnancy. Both pregnancy and hCG treatments are important in inhibiting the development of breast cancer. The treatment of young virgin rats with human chorionic gonadotrophin (hCG), which produced effects similar to a full-term pregnancy, induced the profuse lobular development of the mammary gland, reduced the proliferative activity of the mammary epithelium, and induced inhibin synthesis a secreted protein with tumor-suppressor activity (1). Inhibins are members of the transforming growth factor β superfamily, which modulate the growth and differentiation of several cell types in a variety of target tissues (2). Inhibin is a 32-kDa heterodimer, composed of an α and one of two β subunits, known as βA and βB, which are denoted as inhibin A and B, respectively (2,3). The dimerization of the two inhibin β subunits gives rise to activin A (βA-βA), B (βB-βB) or AB (βA-βB) (3). Inhibin decreases the biosynthesis and release of FSH and antagonizes the action of activin in tumorigenesis, while with activin the reverse applies. Therefore, inhibin may act as a gonadal tumor suppressor, while activin may promote tumor growth (4,5). Inhibin-α has been demonstrated to be a sensitive marker for the majority of sex cord-stromal tumors of the ovary (5). Inhibins are produced by the mammary gland, where they act as paracrine and autocrine growth factors under many physiological and pathological circumstances (6), but, its possible role in the breast is unclear. HCG is a glycoprotein hormone, consisting of two non-covalently linked subunits (α and β), with the free β subunit being the main form produced by non-trophoblastic tumors (7). Many small peptide hormones have been identified as being strongly expressed in cancer, with potential uses in therapeutic intervention or as diagnostic or prognostic biomarkers (8). Until now, only tamoxifen has shown some preventive activity (8), but, hCG has recently shown some promise. Although the functional impact of these overexpressed proteins is unclear, their clinical potential is starting to be realized. These observations led to the suggestion that inhibin-α and β-hCG may be useful in the prevention and hormonal treatment of breast carcinomas. Therefore, it is suggested that the frequency of inhibin-α and β-hCG expressions in breast cancer is correlated with specific tumor features or the prognosis.
This study examined the expressions of inhibin-α and β-hCG in 334 patients, in whom the clinical features and pathologic types had been characterized. The expression of inhibin-α was compared with those of β-hCG, estrogen receptor (ER), progesterone receptor (PR) and HER-2/neu, as well as with the biological parameters, the patient's age, the tumor type, grade and size, lymph node status and tumor recurrences.
Go to : 
MATERIALS AND METHODS
A total of 334 women underwent either a lumpectomy or mastectomy for breast cancer at the Our Lady Mercy Hospital and Uijeongbu St. Mary's Hospital, between 1998 and 2002. 334 formalin-fixed, paraffin embedded tissue blocks were selected. The following information was obtained from the patients' medical records: age, type, grade and size of tumor, lymph node status and tumor recurrences. Two of the authors independently reviewed all the cases, without any prior knowledge of the patient's status, with five cases of an apocrine carcinoma reviewed by Prof. Geung H Ahn, of the Samsung Medical Center, Sungkyunkwan University. The tumor types were classified as follows: infiltrating ductal carcinomas including atypical medullary carcinomas, intraductal carcinomas, lobular tumors including infiltrating lobular carcinomas and lobular carcinomas in situ, apocrine carcinomas and other types, such as medullary carcinoma, mucinous carcinomas, secretory carcinomas and an adenoid cystic carcinoma. The tumors were graded according to the modified Scarff-Bloom-Richardson system (9). In situ lesions, mucinous carcinomas and secretory carcinomas, etc. were categorized as being nongraded. Four cases of intraductal apocrine carcinomas were categorized as being nongraded, with one invasive apocrine carcinoma as grade II (10).
1) Immunohistochemical (IHC) analyses
IHC analyses for the inhibin-α (1:50, Clone R1, Dako, Carpinteria, CA), β-hCG (1:100, Clone CG04, NeoMarkers, CA), ER (1:100, Dako, Glostrup, Denmark), PR (1:100, Dako, Glostrup, Denmark) and HER-2/neu (1:1,000, Dako, Glostrup, Denmark) oncogenes were performed on the formalin-fixed, paraffin-embedded materials. The standard avidin-biotin-peroxidase complex (ABC) technique was used, according to the manufacturer's instructions. In order to eliminate endogenous biotin as a possible source of any nonspecific staining, a biotin solution was added to the primary antibody. After retrieving the antigen in citrate buffer at pH 6.0, and blocking the endogenous peroxidase activity in 3% alcoholic hydrogen peroxide, the sections were incubated for 15 min before the addition of the primary antibody in an avidin solution. Ovarian and placental tissues for inhibin and hCG were used as the positive controls.
2) Immunohistochemical (IHC) interpretation
The IHC results were independently interpreted by two of the authors. Inhibin staining was regarded as positive if more than 5% of the tumor cells showed cytoplasmic staining (3,11). The normal ducts showed negative staining. HCG immunostaining was interpreted as being positive when the tumor cells displayed cytoplasmic staining (12,13). The staining for ER and PR was considered negative when there were no nuclear-positive stained tumor cells. The staining was considered positive when more than 10% of the tumor cells showed positive nuclear staining. Breast carcinomas that scored positive (+++) and negative (-/+) with the HercepTest (Dako) for HER-2/neu were used as the positive and negative controls, respectively. Only the membrane staining pattern and intensity of the invasive tumor cells were scored. The adjacent normal epithelial cells showed negative staining. The immunoreactivity for HER-2/neu was defined as positive if >10% of the tumor cells showed weak to moderate complete membrane staining (2+) or strong complete membrane staining (3+). The reaction was considered negative (0/1+) when the membrane staining was absent or present in <10% of tumor cells (14).
3) Statistical analysis
A statistical analysis was performed using the SPSS for Windows software (Version 8.0; SPSS, Chicago, IL). The Pearson X2-test was used to compare categorical variables. Two-sided p values < 0.05 were considered significant.
Go to :
RESULTS
Table 1 shows the clinicopathological characteristics and IHC expressions.
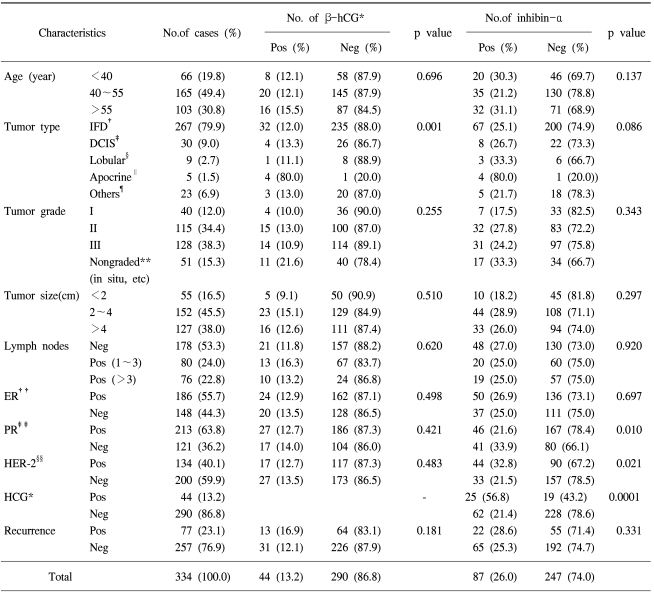
Table 1
Tumor characteristics, the relationships between β-hCG and inhibin-α expression and the clinicopathological variables, ER, PR and HER-2
*human chorionic gonadotrophin, †infiltrating ductal carcinoma, no specific type, ‡intraductal carcinoma, §infiltrating lobular carcinoma and lobular carcinoma in situ, ∥apocrine carcinoma, ¶medullary, mucinous, secretory and adenoid cystic carcinoma, **in situ lesions, mucinous and secretory carcinoma, ††estrogen receptor, ‡‡progesterone receptor, §§Her-2/neu oncogene.
![]()
1) IHC expression for inhibin-α
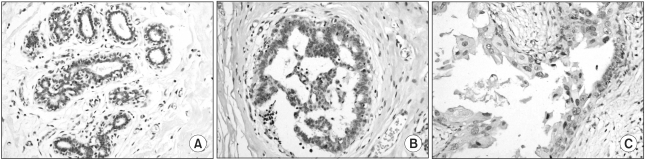
Using immunohistochemistry, inhibin-α was found to be expressed in eighty-seven cases (26.0%). Positive staining was focal in some cases, but diffuse in others. Inhibin-α was found to be positively expressed in 25.1% of infiltrating ductal carcinomas (67/267), 26.7% of intraductal carcinomas (8/30), 33.3% of lobular tumors (3/9), 80.0% of apocrine carcinomas (4/5) and 21.7% of the other types (5/23). Inhibin-α was negatively expressed in the cytoplasm of the normal ductal epithelial cells (Fig. 1A) and intraductal hyperplasia (Fig. 1B) of the same case, but apocrine epithelial cells showed a weakly positive reaction (Fig. 1C). Negative (Fig. 2A) or moderately positive inhibin-α expression was observed in the conventional ductal carcinomas, and intensely positive expression (Fig. 2B) was found in the apocrine carcinomas.
2) IHC expression for β-hCG
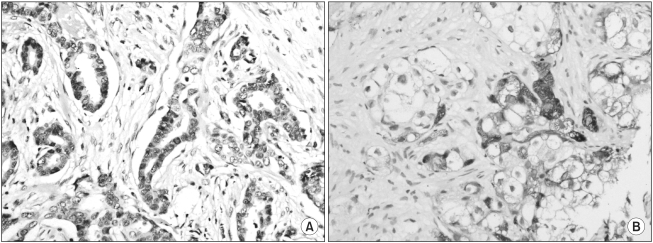
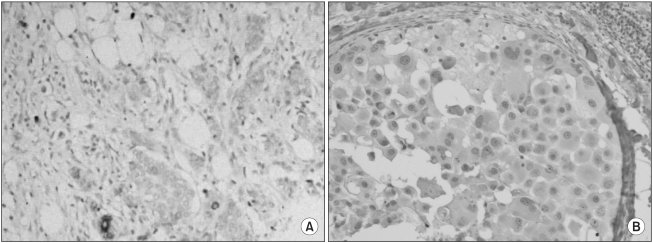
Of the 334 cases, 44 cases (13.2%) showed positive expression. HCG was expressed in 32 of the 267 infiltrating ductal carcinomas (12.0%), 4 of the 30 intraductal carcinomas (13.3%), one of the 9 lobular tumors (11.1%), 4 of the 5 apocrine carcinomas (80.0%) and 3 of the 23 other types (medullary, mucinous, secretory and adenoid cystic carcinomas) (13.0%). HCG was focally expressed in the cytoplasm of the conventional type tumor cells (Fig. 3A). However, the apocrine type displayed diffusely strong cytoplasmic staining (Fig. 3B). HCG expression was negative in the cytoplasm of the normal ductal epithelial cells and intraductal hyperplasia.
3) Relationships between inhibin-α and β-hCG expression and the clinicopathological characteristics, ER, PR and HER-2/neu oncogene
Inhibin-α expression was significantly correlated with β-hCG (p<0.0001), PR (p=0.010) and HER-2/neu (p=0.021), but not with the patient's age (p=0.137), tumor type (p=0.086), tumor grade (p=0.343), tumor size (p=0.297), lymph node status (p=0.920), ER (p=0.697) and tumor recurrence (p=0.331). HCG expression was correlated with the histological tumor types (p=0.001), but not with the patient's age (p=0.696), tumor grade (p=0.255), tumor size (p=0.510), lymph node status (p=0.620), ER (p=0.498), PR (p=0.421), HER-2/neu oncogene expression (p=0.483) and tumor recurrence (p=0.181).
Go to :
DISCUSSION
Inhibin-α expression in human breast tissue was examined using a monoclonal antibody specific to the α inhibin subunit (clone R1, 1~32 amino terminal peptides). Inhibin-α immunoreactivity was negative in the cytoplasm of normal ductal epithelial cells and intraductal hyperplasia of the same case. However, the apocrine epithelial cells showed a positive reaction. The results showed that Inhibin-α was up-regulated in 26.0% of the breast carcinomas and in 25.1~26.7% of the conventional ductal carcinomas. However, the apocrine type displayed higher cytoplasmic staining than the other types, with up to 80.0%. In contrast, Reis et al. (6) detected inhibin βA subunit mRNA in normal mammary tissue using a reverse transcription polymerase chain reaction (RT-PCR). In addition, other authors, using another types of antibodies, have reported moderately positive inhibin-α expression in benign epithelial cells, intense positive expression in apocrine epithelial cells of fibrocystic disease, and weak to moderate expression in neoplastic cells (3,15). However, Risbridger et al. demonstrated that inhibin-α was not expressed in normal prostate ductal epithelial cells, which concurs with the present results. They used the same antibody clone R1, as used in this study. They reported that inhibin α was up-regulated from 23 to 66% in prostate carcinoma patients in four independent laboratories (11). An important difference related to the antibodies used in these studies. The most commonly used inhibin α antibody is the Groome R1 antibody raised to the amino acids 3~24 of the inhibin α (11,16). The results of this study did not support the previous evidence that inhibin α was down regulated in breast cancer (6), but agreed with those reported by Risbridger et al. (11). The up-regulation of inhibin α would indicate a more advanced disease status and metastasis. A patient with prostate cancer whose tumor tissue had a more elevated inhibin α expression had a higher risk of recurrence (11). Their study concluded that inhibin α was frequently over-expressed in high-grade prostate cancers (11). Therefore, the tumor suppressor activities of inhibin α would dominate in non-malignant tissue, but its oncogenic and pro-metastatic activities would eventually emerge (11). The prognostic significance of inhibin α in this study was its significant correlation with β-hCG, PR and HER-2/neu. The role of activin and inhibin as endocrine and/or paracrine factors in the breast is unclear. It is currently believed that inhibin antagonizes the action of activin by interacting, via accessory binding proteins (e.g. betaglycan), to compete with the activin receptors (17).
HCG expression has been described in nongestational carcinomas, and has been found in 10~37.4% of breast tumors (7,13,18). In this study, 44 cases (13.2%) showed positive expression. HCG in the nonapocrine type was expressed in 11.1 to 13.3% of cases, but was found in 80.0% of those with the apocrine type. These results demonstrate that hCG overexpression may help improve the diagnostic accuracy when breast carcinomas are found showing apocrine differentiation. HCG induces the maturation of the breast, where the differentiated gland has a lower proliferative activity and a more efficient mechanism of DNA repair (8). Therefore, the preventive effect of hCG on experimental mammary carcinogenesis can be attributed to the inhibition of cell proliferation, the increased DNA repair capabilities of the mammary epithelium, the decreased binding of the carcinogen to the DNA and the activation of programmed cell death genes that lead to apoptosis (19). A direct role for hCG in the differentiation of breast tissue is evidenced by the presence of the hCG receptor in normal breast tissue. Other hypotheses suggest an indirect effect of hCG through its paracrine product, inhibin (8). These results suggest that hCG plays an indirect, but important role in inhibiting further cell proliferation in relation to inhibin. Currently, ectopic β-hCG expression is not only important for research in tumor biology, but also in therapeutic trials (7).
Go to :
 XML Download
XML Download