

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Maspin is a recently identified 42-kDa protein, which belongs to the serine protease inhibitors (serpin) family, and shares extensive homology with PAI (plasminogen activator inhibitor)-2 and other serpins (1). The Maspin gene was originally identified in normal mammary epithelium by subtractive hybridization on the basis of its expression at the mRNA level (1). The Maspin gene has been localized to chromosome 18q21.3, which includes PAI-2 and the squamous cell carcinoma antigens 1 and 2 (2). The 1 kb promoter region of the Maspin gene contains binding sites for several important transcription factors, such as Ets, Ap1, HRE and p53 (3).
Although Maspin has been considered as a tumor suppressor that inhibits the motility, invasiveness and metastasis of breast and prostate cancer cells (4~6), conflicting findings on the expression of Maspin, and its association with cancer prognosis, have been reported. Maspin seems to behave as an oncogene, rather than a tumor suppressor gene, in pancreatic, ovarian, thyroid, breast cancers and melanomas (7~12). Maspin expression was observed in 23 of 24 tumor specimens obtained from pancreatic cancer patients, and in 5 of 9 pancreatic cancer cell lines, but not in normal pancreatic tissues (7). Maspin expression was also observed in all of the 72 pancreatic ductal adenocarcinomas examined, whereas faint or no expression was observed in the corresponding normal pancreatic tissues (8). In a Cox proportional hazard model, high Maspin expression predicted a high hazard rate (8). Patients with invasive ovarian cancer exhibiting Maspin up-regulation showed worse prognoses (9). Ogasawara et al. demonstrated that expression of Maspin by DNA hypomethylation was closely associated with the morphological dedifferentiation in thyroid cancers (10). In mammary ductal adenocarcinomas, the expression of Maspin is up-regulated during their progression (11,13), in contrast to the previous reports of Zou et al. (1) and Sheng et al. (4).
Maspin protein expression was also found in 1 of 5 melanoma cell lines, with positive immunoreactivity for Maspin in 5 of 40 melanomas (12.5%), while normal melanocytes and 40 melanocytic nevi were negative (12).
Maspin expression has been reported to be regulated by epigenetic modification in a cell-type-specific manner, and inversely correlated with the methylation status of the Maspin promoter (14). This cell-type-specific regulation mechanism may contribute to paradoxical Maspin expression among cancers (10,14). Maspin expression, and its functional significance, has not been fully elucidated in human gastric cancer. There have been conflicting reports about Maspin expression during carcinogenesis and in the prognosis of gastric cancer (7,15~18).
To investigate the expression pattern of Maspin in human gastric cancer, and its possible correlation with clinicopathological findings, the levels of Maspin mRNA and protein expressions were investigated in gastric adenocarcinomas and normal gastric mucosa.
Go to : 
MATERIALS AND METHODS
1) Tissues and cell lines
Sixty two grossly evident cancer tissues were obtained by surgical resection, and 31 noncancerous gastric tissues at proximal resection margin, were included for comparison. A portion of fresh normal tissue was used for H&E staining to evaluate the presence of tumor cells and dysplasia. After the histological diagnosis, the tissues were immediately stored at -80℃. The remaining tissues were fixed in 10% formalin, and then embedded in paraffin for routine histological processing and immunohistochemical study. Paraffin blocks for the immunohistochemical study were taken from tissues composed of both cancer and adjacent normal mucosa. All the clinicopathological parameters, including tumor size, Lauren classification, vascular invasion, depth of tumor invasion, lymph node metastasis and stage, were evaluated according to the AJCC cancer staging manual (19). Of the 62 gastric carcinomas, 6 and 56 were early and advanced gastric carcinomas, respectively. Sixteen, 12, 26 and 8 tumors were stages 1, 2, 3 and 4, respectively. Histologically, 27 and 35 were intestinal and diffuse types, respectively (20). Four human gastric cancer cell lines (SNU-719, SNU-484, SNU-620 and MKN-74) were obtained from KCLB (Seoul, Korea). All of cancer cell lines were cultured in RPMI 1640 (Gibco BRL, Gaithersburg, MD), supplemented with 10% FCS.
2) Nested RT-PCR
Total RNA was extracted from 50~100 mg of the 60 frozen gastric cancer tissues, 31 normal tissues and the human gastric cancer cell lines, using Trizol reagent, according to the manufacturer's protocol (Gibco BRL). Following the addition of 1 ml Trizol reagent, the tissues were homogenized using homogenizer (Polytron, Switzerland). The cDNA was synthesized using 2 µg of total RNA in 25 µl of reaction mixture, containing 50 mM Tris-HCl (pH 8.3), 75 mM KCl, 3 mM MgCl2, 10 mM DTT, 0.5 mM of each dNTP, 200 U of M-MLV reverse transcriptase (Promega, Madison, WI), 25 U RNase inhibitor and 1 µg of oligo (dT)15 primer, at 37℃ for 1 hour. Nested RT-PCR of maspin was performed using the following primers: (a) 5'-CACTGGGCAATGTCCTCTTC-3' (sense), (b) 5'-TGGTCTGGTCGTTCACACTG-3' (antisense), (c) 5'-CTCTCCAATCTGTCTCTCCACC-3' (sense), and (d) 5'-GGTCGTTCACACTGTTGTCAGC-3' (antisense). The first amplification was performed using primers (a) and (b), and the reaction mixture [containing 10 mM Tris-HCl (pH 9.0), 50 mM KCl, 0.1% Triton X-100, 1.5 mM MgCl2, 200 µM each of dNTPs, and 1.25 U of Taq polymerase (Promega)] for 35 cycles (1 min at 94℃, 1 min at 55℃ and 1 min at 72℃). Then, 1 µl of the first-round PCR products was used for the second-round PCR with primer (c) and (d). Amplification of the second-round PCR was performed for 30 cycles (1 min at 94℃, 1 min at 60℃ and 1 min at 72℃). The housekeeping gene, glyceraldehyde-3-phosphate dehydrogenase (GADPH), was used as an internal control; the primers for GADPH were as follows: 5'-ATCCCATCACCATCTTCCAG-3' (sense) and 5'-GCCATCACGCCACAGTTTCC-3' (antisense). Amplification of the GADPH was performed for all samples under the same condition as the first-round of PCR of maspin. To perform parallel PCR amplification of the maspin mRNA, the samples were compared with the intensity of the GADPH PCR products, using the Bio-1D program (Vilber Lourmat, France), with the same amount of cDNA as used for the first PCR of Maspin. The Maspin mRNA expression in four human gastric cancer cell lines, SNU-719, SNU-484, SNU-620 and MKN-74, was also analyzed. The PCR products were subjected to electrophoresis on 2% agarose gel. Following the electrophoresis, the gels were stained with 0.5 mg/ml ethidium bromide, photographed and analyzed using an image analysis system (Vilber Lourmat, France)
3) Immunohistochemical analysis
The immunohistochemical studies were performed using the immunoperoxidase technique employing the mouse anti-human Maspin monoclonal antibody (clone G167-70, 1:1,000, Pharmingen, San Diego, CA). Briefly, 5 µm sections of formalin-fixed, paraffin-embedded tissues were deparaffinized in xylene and rehydrated through a series of graded alcohol. The sections were submerged in 10 mM citrate buffer and placed in a microwave oven for 10 minutes, twice. The slides were incubated with primary antibody, in phosphate buffered saline (PBS), and 1% bovine serum albumin, overnight at 4℃. After incubation with the primary antibody, the avidin-biotin complex method (LSAB kit; DAKO, Carpinteria, CA), with 3-3'-diaminobendizine-tetrachloride (Biogenex, San Ramon, CA) as a chromogen, was used, and the slides counterstained with Meyer's hematoxyline. The negative control was provided by incubation with saline instead of the primary antibody, with benign breast parenchymal tissue used as a positive control. The immunostained slides were evaluated by estimating the percentage of positive cells (proportion score) and staining intensity (intensity score), as described by Song et al., but with some modifications (21). In brief, the proportion scores were graded as 0 when no immunoreactive cells were observed, and as levels 1, 2, 3, 4 and 5 when the numbers of immunoreactive cells were less than 5, 10, 40 and 70% and more than 70%, respectively. The intensity scores were grade as 0 when there was no immunoreactivity and as 1, 2 and 3 when the representative staining intensities were weak, intermediate and strong, respectively. The final estimation of the immunoreactivity was assesses as negative if the summation of the proportion and intensity scores was lower than 4 and as positive if the summation was within the range 4 to 8.
4) Statistical analysis
Statistical analysis was performed with the Pearson chi-squared test using the BMDP program; p<0.05 was considered as statistically significant.
Go to :
RESULTS
1) Expression of maspin mRNA
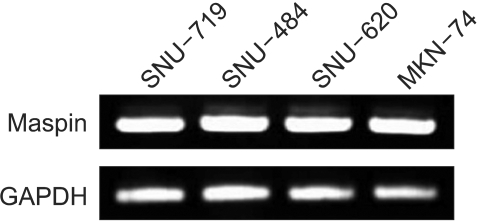
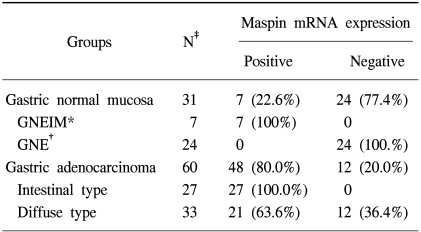
Maspin mRNA was detected in 48 of the 60 (80.0%) gastric carcinoma tissues, whereas only 7 of the 31 (22.6%) normal mucosa were positive (p<0.001) (Fig. 1, Table 1). The positive rate of Maspin mRNA expression was significantly higher in the intestinal type of adenocarcinoma than the diffuse type adenocarcinoma [100.0% (27/27) vs. 63.6% (21/33), p<0.05] (Table 1). Maspin mRNA expression was detected in all four of the gastric cancer cell lines, SNU-719, SNU-484, SNU-620 and MKN-74 (Fig. 2).
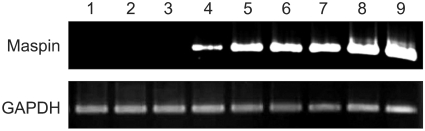 | Fig. 1Expressions of maspin mRNA in normal gastric mucosa (lane 1~4) and gastric adenocarcinoma tissues (lane 5~9) using nested RT-PCR. One normal gastric mucosa (lane 4) was weakly positive. GADPH was used as an internal control.
|
2) Expression of Maspin protein
In the immunohistochemical assay, the expression of Maspin protein was found in 39 of the 62 (62.9%) gastric adenocarcinoma tissues. In contrast, 17 of the 62 (27.4%) noncancerous gastric mucosa adjacent to carcinoma cells were positive for Maspin protein (Fig. 3). Positive staining was mainly cytoplasmic, with occasional nuclear staining. The noncancerous gastric mucosa adjacent to gastric cancer revealed intestinal metaplasia in 44 samples. Interestingly, immunohistochemical positivity of Maspin was observed in only the normal gastric epithelia with intestinal metaplasia (GNEIM). Therefore, the positive rate of Maspin protein expression was significantly higher in adenocarcinoma than in the normal gastric tissue (62.9% vs. 27.4%, p<0.05). All the gastric glands and gastric normal epithelia without intestinal metaplasia (GNE) were negative for Maspin protein. Maspin protein expression was not observed in the inflammatory cells, including the lymphocytes and other stromal components.
 | Fig. 3Immunohistochemical staining for Maspin in gastric adenocarcinomas. (A) Maspin was strongly expressed in the intestinal type (arrow). No staining was seen in normal non-metaplastic gastric mucosa (arrow head). Immunohistochemical stain, original magnification ×100. (B) Maspin was negative in the diffuse type of gastric adenocarcinoma (arrow). Maspin immunostaining was observed in the intestinal metaplastic epithelium (arrow head). Immunohistochemical stain, original magnification ×100.
|
3) Correlation between Maspin expression and clinicopathological findings
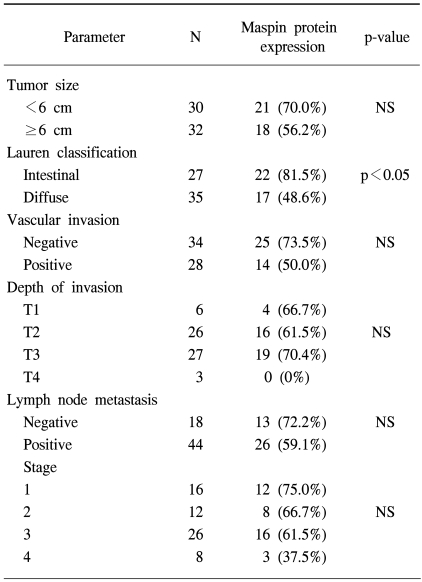
Comparing the relationship of Maspin expression with the clinicopathological findings (Table 2), Maspin protein expression was more frequently found in the intestinal (22/27, 81.5%) than diffuse type (17/35, 48.6%) (p<0.05) (Fig. 3). There was no significant correlation between Maspin expression and the other parameters, i.e., tumor size, vascular invasion, invasion depth, lymph node metastasis and tumor stage.
Go to :
DISCUSSION
Gastric cancer is one of the most common malignancies in Korea. Although there have been many reported studies about the carcinogenesis and progression of gastric cancer, the molecular aspects remain unknown (22~25). Maspin was originally described as a tumor suppressor that affects cell motility (1). Maspin expression has rarely been evaluated in human gastric cancers, but has shown conflicting results. Maass et al. failed to detect Maspin mRNA in 6 gastric cancer cell lines using Northern blot analysis (7). However, Akiyama et al. demonstrated that Maspin was overexpressed in 3 of 4 gastric cancer cell lines with hypomethylation, at either both alleles or a haploid allele (15). Using an RT-PCR approach, the Maspin mRNA was revealed to be expressed in all of four gastric cancer cell lines in this study.
Akiyama et al. demonstrated dense and diffuse immunoreac tivity for Maspin in 40 of 50 (80%) gastric cancers and all GNEIM, but not in GNE (15). Son et al. reported in an immunohistochemical study that Maspin was frequently overexpressed in gastric adenocarcinomas, regardless of the histological type, and in GNEIM also, but not in GNE (16). With the use of a DNA microarray, the expression of Maspin was found to correlate with lymph node metastasis in gastric cancer (17). However, Wang et al. reported contradictory results in that Maspin was expressed in normal (79.8%), dysplastic (75.4%) and carcinoma (50.4%) tissues of the stomach, but found more frequent Maspin expression in the intestinal (66.7%) than diffuse type (42.1%)(18). In our immunohistochemical study, all the GNE and gastric glands exhibited negative staining for Maspin, whereas GNEIM showed weak, but generally positive, staining. Unlike Son's results, in this study, that the rate of Maspin expression was found to be significantly higher in the intestinal than diffuse type. The molecular and biological mechanisms underlying these conflicting results on the function of Maspin as oncogene or suppressor gene are not fully understood. Futscher et al. demonstrated that the Maspin expression of normal cells was regulated by epigenetic modifications in a cell-type-specific manner, which was inversely correlated with the methylation status of the Maspin promoter (14). The Maspin gene promotor region of all GNE was hypermethylated on both alleles, whereas GNEIM frequently represented the haploid type of hypomethylation status, and demethylation frequently occurred and extended to both alleles in gastric cancer (15). This cell-type-specific regulation mechanism may contribute to paradoxical Maspin expression among cancers and organs. Also, the reason for the discrepancy between the positive rate for mRNA and protein expressions might possibly be that mutational alteration of the Maspin gene, or increased expressions of certain inhibitory factors, affects the expression level of Maspin protein in gastric cancer cells. Gastric intestinal metaplasia, an intermediate step in Correa's cascade of gastric carcinogenesis, is generally regarded as a pre-malignant lesion (24). Mutoh et al successfully showed that long-term intestinal metaplasia induced invasive gastric cancer in Cdx2-transgenic mice (25). Our results suggested that Maspin expression might be associated with the carcinogenesis of gastric adenocarcinomas, especially of the intestinal type. Further investigations will be required to determine the mechanism, and the clinical significance, of higher Maspin expression in GNEIM and the intestinal type of gastric adenocarcinomas.
Go to :
CONCLUSIONS
Maspin mRNA and protein are more frequently expressed in gastric adenocarcinoma than in normal gastric tissues. The positive rates of Maspin mRNA and protein expressions were significantly higher in the intestinal type of adenocarcinoma than in the diffuse type. Collectively, our data demonstrate that Maspin is frequently expressed in gastric adenocarcinomas, and its expression might be implicated in the development of the intestinal type of gastric adenocarcinoma.
Go to :
 XML Download
XML Download