

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Gastric adenocarcinomas have been the leading cause of cancer death worldwide throughout most of the twentieth century (1), and are now ranked as the primary cause of cancer death in Korea and the second leading cause of cancer death in the world (2). The only proven, potentially curative treatment for this disease is surgical resection; for both the gross and microscopic disease. Even after a curative gastrectomy, the disease still recurs in both regional and distant sites in 50~80% of the patients (3). Some patients have no chance to receive an operation due to the far advanced progression of their gastric cancer.
In these relapsed or far advanced cancer patients, a curative resection is rarely possible; therefore, effective palliative chemotherapy or other systemic therapies are required for disease control.
Many chemotherapeutic agents have been studied for the treatment of gastric cancer since the late 1970s. Of these drugs, cisplatin has been proved to be effective for treating gastric adenocarcinomas; the response rates between 30~60% have been reported when combined with 5-fuloruracil (5-FU) (4~6). Despite the effectiveness of cisplatin, it has some serious toxicities, such as nause/vominting, nephrotoxicity and neurotoxicity. To overcome these drawbacks, heptaplatin (SKI-2053R), a new derivatives of platinum, has been developed (7,8). The initial phase II single agent heptaplatin study for advanced gastric carcinomas showed some promising results, with minimal toxicities and an efficacy comparable to cisplatin (9).
Several studies have suggested that the biochemical modulation of 5-FU by leucovorin (LV) should confer a superior response rate compared to 5-FU alone for advanced gastric cancer (10), although the most effective dosage and mode of administering LV remain to be documented. Based on these findings, we have conducted a single center phase II trial of a heptaplatin, 5-FU and LV combination chemotherapy for advanced gastric cancer, with the results reported herein.
MATERIALS AND METHODS
1) Eligibility
Between January 2001 and March 2003, thirty-one patients were enrolled in this trial study. The eligibility criteria were as follows: (1) a histologically proven gastric adenocarcinoma with one or more measurable lesions, (2) a WHO performance status of 3 or less; adequate hematopoietic, hepatic and renal functions, and (3) no previous palliative chemotherapy. For those patients who had received previous adjuvant chemotherapy more than 6 months after the completion of their adjuvant therapy (4), and if they had received no prior radiation therapy (5), were then also enrolled into the study. The informed, written consent was obtained from all the subjects.
2) Treatment schedule
The eligible patients were treated as follows: heptaplatin, 400 mg/m2/day, was intravenously administered (IV) over a period of 1 hour on day 1; this was given along with adequate, vigorous hydration before and after treatment. 5-FU, 800 mg/m2/day was IV administered over a 12 hour period on days 1 to 5. Leucovorin, 30 mg (a fixed dose), was administered as an IV bolus before the 5-FU infusion. The cycles were repeated every 3 weeks.
3) Dose modifications for toxicity
The prerequisites for dose modifications were as follows: (1) any episode of grade 4 neutropenia of more than 7 days' duration, (2) any episode of febrile neutropenia (3), any grade 4 thrombocytopenia and (4) any nonhematologic grade 3 or 4 toxicity, excluding nausea/vomiting and alopecia. The dose modification criteria were designed as follows: (1) for the above conditions, the dose of 5-FU was reduced by 20% in the subsequent cycles, (2) for neuropathy ≥ grade 3, the treatment was interrupted, (3) for nephropathy ≥ grade 3, the treatment was withheld until recovery (a serum creatinine level <1.5 times the upper normal value, and proteinuria ≤1+) and then treatment was started again with a 20% heptaplatin dose reduction. If the blood counts did not recovered to an absolute neutrophil count ≥1,500/ul, and the platelet count was ≥100,000/ul on the day of therapy, the treatment was further withheld until recovery. After a maximum delay of two weeks, no further therapy was administered.
4) Pretreatment, follow-up studies and response evaluation
Pretreatment evaluations were performed by taking a complete history and physical examination (P/E), documenting the performance status, a pretreatment laboratory evaluation (full blood counts, biochemical tests, urinalysis and viral hepatitis markers), a 12-lead electrocardiogram and chest radiography. Blood counts and biochemical tests were performed every 3 weeks prior to treatment initiation. Urinalysis was performed when the patients complained of fatigue or there was a poor oral intake, hypoalbuminemia or newly developed non-hematological toxicities >grade 1 after each cycle of therapy. Tumor measurements were performed by a specific radiograph test that documented the measurable disease before treatment. The treatment response was evaluated after every two cycles of therapy. The tumor response classification was derived from the RECIST criteria. Toxicity was graded according to the WHO scoring system. Treatment was stopped if the disease progressed, if grade 4 toxicity occurred, excluding hematological toxicities and nausea/vomiting, if the ECOG performance status of the patient was 4 or if they refused further treatment.
5) Statistical analysis
Patients who had received at least one cycle of treatment were assessable for toxicity evaluation. The response duration was measured from the onset of PR (even if patient later had a CR) until there was evidence of PD. Time to progression (TTP) was calculated from the start of treatment until there was evidence of PD; actuarial survival was measured from the start of treatment until the last follow-up or death. The 95% confidence interval (CI) for the response rate (RR) was calculated from the binomial distribution. The overall survival was calculated by the Kaplan-Meier method. The sample size was calculated to accept the hypothesis that 'the true RR is at least 40%' with an alpha=0.1 and a beta=0.2, according to Simon's optimal design (11).
RESULTS
1) Patient characteristics
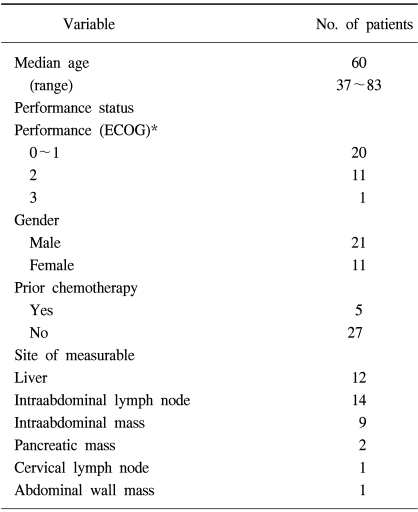
The characteristics of the thirty-two patients enrolled in this study are listed in Table 1. All patients received at least one cycle of chemotherapy, and were assessable for treatment toxicity, with 26 patients receiving at least two cycles of treatment, who were also assessable for treatment response. Of the six non-assessable patients, five refused further treatment and one died of pneumonia in a neutropenic state. Of these six patients, two had received prior adjuvant chemotherapy. Of the 5 patients who refused further treatment and two had grade 4 neutropenia, one had grade 3 nausea/vomiting; one also had no definite toxicity, with the exception of anorexia and general weakness.
2) Response to treatment and survival
Among the 26 assessable patients, there were one CR and nine PRs, with an overall RR of 38% (95% CI, 19~57%); there were also 7 SDs (27%; 95% CI, 10~44%) and 9 PDs (46%: 95% CI, 27~65%). When the response rate was calculated by an intention to treatment analysis, the RR was 31%. The median follow-up period, time to disease progression and overall survival were 18 (range: 3~85 weeks), 15 (range: 3~85 weeks) and 33 weeks (range: 536 weeks), respectively (Fig. 1). The median remission duration for the 10 responding patients was 20 weeks (range: 11~60 weeks).
3) Toxicities
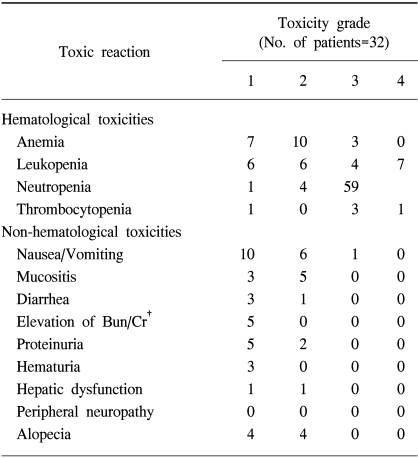
The hematological and non-hematological toxicities encountered in this study were evaluated for all patients, and are shown in Table 2. The grade III-IV toxicities that developed included neutropenia in 14 patients (44%) and neutropenic fever in 5 patients (16%). Of these, one elderly patient, with an ECOG performance II, who had massive lymphadenopathy in the abdomen, developed severe neutropenia after the first round of chemotherapy, which was followed by pneumonia and sepsis. The patient died of sepsis, in a neutropenic state, even though the patient was aggressively managed with broadspectrum antibiotics and G-CSF.
No definite neuropathy was observed. Grade I-II nephropathy was observed: grade I high BUN/creatinine levels in 5 patients (16%), but the levels were normalized after hydration; grade II proteinuria in 2 (6%), grade I proteinuria in 5 (16%), and grade I hematuria in 3 (9%).
4) Compliance with treatment
A total of 124 treatment cycles were administered (a median of 3 cycles; range of treatment cycles: 1~6 cycles), with a mean of 3.88 cycles per patient. The planned six cycles were not completed for the patients due to the following reasons: PD (15 patients); SD with persisting symptoms and poor performance (two patients after 4 cycles); personal choice for reasons unrelated toxicities or disease progression (4 patients); and toxic death (one patient). Eleven patients required a dose reduction and eighteen had delays in their chemotherapy of 1 week or more. More than a 1 week delay occurred in four patients. The administered mean dose intensity for heptaplatin and 5-FU were 0.78 (range: 0.52~1.04) and 0.82 (range: 0.52~1.10), respectively.
DISCUSSION
In this study trial, the combination chemotherapy of heptaplatin and 5-FU displayed good clinical activity, with well-tolerated toxicities. The response rates were comparable to those of previously reported results for the combination chemotherapy of 5-FU and CDDP (6,12), and 5-FU and oxaliplatin (13,14); this suggests that the efficacy of heptaplatin is as good as that of CDDP and oxaliplatin.
The toxicity profiles of heptaplatin and 5-FU were not very serious. The most common toxicity greater than grade II was neutropenia. 5 of the 14 neutropenic patients developed neutropenic fever, yet this was well controlled by empirical antibiotics and G-CSF administration, except in one patient. The most common non-hematological toxicity greater than grade II was nausea/vomiting. However, only one of 32 patients developed Grade III nausea/vomiting. Given the previous studies on the cisplatin and 5-FU regimens produced greater than grade III nausea/vomiting in a larger proportion of patients (6,12), heptaplatin was observed to be well-tolerated in terms of nausea/vomiting. A phase II trial of heptaplatin for advanced stomach cancer also showed that the nausea/vomiting was mild and transient (9).
Proteinuria developed in 7 patients (22%), but the incidence was slightly less than that reported in other trials (9,15). This may be attributable to the fact urinalysis was not mandatory for every patient as the proteinuria was transient and completely resolved after treatment, with urinalysis only performed for those cases with a high probability of complications. Azotemia occurred in 5 patients (16%), and this was rapidly normalized in all patients. This result was consistent with other previously reported results (9).
Heptaplatin has been reported to induce less frequent and milder neurotoxicity compared with the other platinum compounds, oxaliplatin or cisplatin (9,16).
In this study, no neuropathy was observed, which when compared to the results of a phase II trial using heptaplatin alone, the incidence of neuropathy was lower in our study. However, no neuropathy was observed in a previously reported pilot study of heptaplatin, UFT-E and leucovorin for stomach cancer (16).

 XML Download
XML Download