

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
The Korea Central Cancer Registry (KCCR) was started as an ambitious project of the Ministry of Health and Welfare in 1980 (1). In the beginning, 47 nationwide resident-training general hospitals participated in this program. The number of participating hospitals and registered malignancies increased year by year, and 134 hospitals submitted their data diskettes in 2001.
In 1996, the International Classification of Diseases for Oncology 2nd edition (ICD-O-2) was translated into Korean and distributed to all the participating hospitals. Topography and Morphology codes of the ICD-O-2 have been used since the 16th annual report of the KCCR.
The aim of this paper is to provide a summary of the 22nd annual report of the KCCR, which was published in February 2003 (1). It contains the relative frequencies of various cancers in the Republic of Korea, derived from the nationwide database of the hospital-based cancer registry program from January 1, to December 31, 2001.
MATERIALS AND METHODS
One hundred and thirty four hospitals participated in the KCCR in 2001. All cancer registry data, submitted from the participating hospitals on diskettes during the year, were reviewed and sorted by qualified cancer registrars in the National cancer Center. After correction of erroneous coding of topography and morphology, cancer cases were classified according to the ICD-O-2. To avoid duplication, the computer compared the personal identification number of all subjects. The software program "IARC Check" which was freely distributed by International Association of Cancer Registry (IACR), was used to evaluate the quality of registered cancer cases. The pathologists working at the hospitals where the cases were diagnosed, reviewed the cases with errors shown from "IARC Check" program. Much emphasis was placed on the basis of diagnosis during this selection procedure. Cases diagnosed by histological examination were preferentially chosen.
Of 111,816 malignancies registered, 10,106 (9.0%) duplicated malignancies were excluded. Among the remaining 95,542 malignancies, 3,598 (3.8%) cases with carcinoma in situ (Morphology code/2) were separated. Finally, 91,944 malignancies were analyzed.
RESULTS
1) Marginal frequency of malignant neoplasm and carcinoma in situ by age, sex, and topography
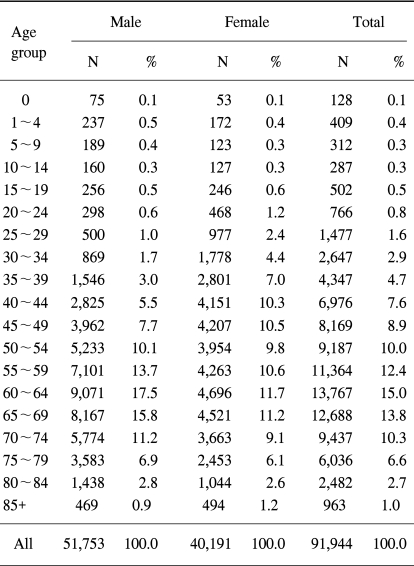
Of the total 91,944 registered malignancies 51,753 (56.3%) cases were males and 40,191 (43.7%) were females. The proportion of cancer cases among children (age 0~14) and among the elderly (65 and more) were 1.1 and 34.4%, respectively (Table 1).
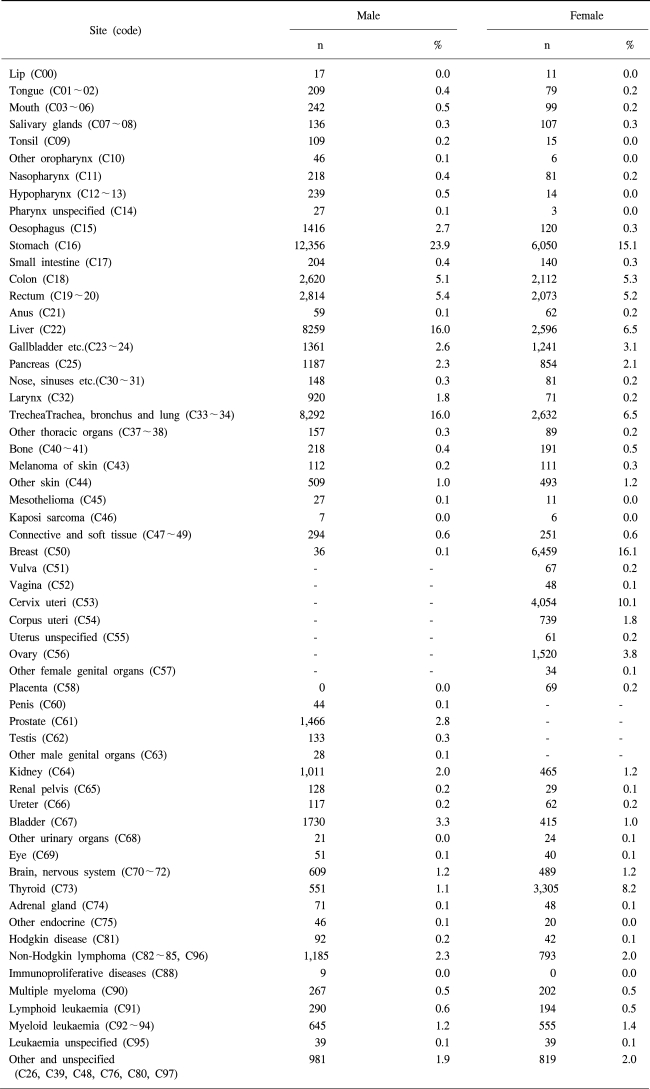
The most common 10 primary sites among males were stomach (24.1%), lung (16.0%), liver (16.0%), colorectum (10.5%), blader (3.4%), prostate (2.8%), esophagus (2.7%), hematopoietic & reticuloendothelial systems (2.7%), pancreas (2.3%), and kidney (2.0%). Among females, they were the breast (16.1%), stomach (15.3%), colorectum (10.5%), cervix uteri (10.1%), thyroid (8.3%), lung (6.6%), liver (6.5%), ovary (3.8%), hematopoietic & reticuloendothelial systems (2.7%), and pancreas (2.1%) (Fig. 1).
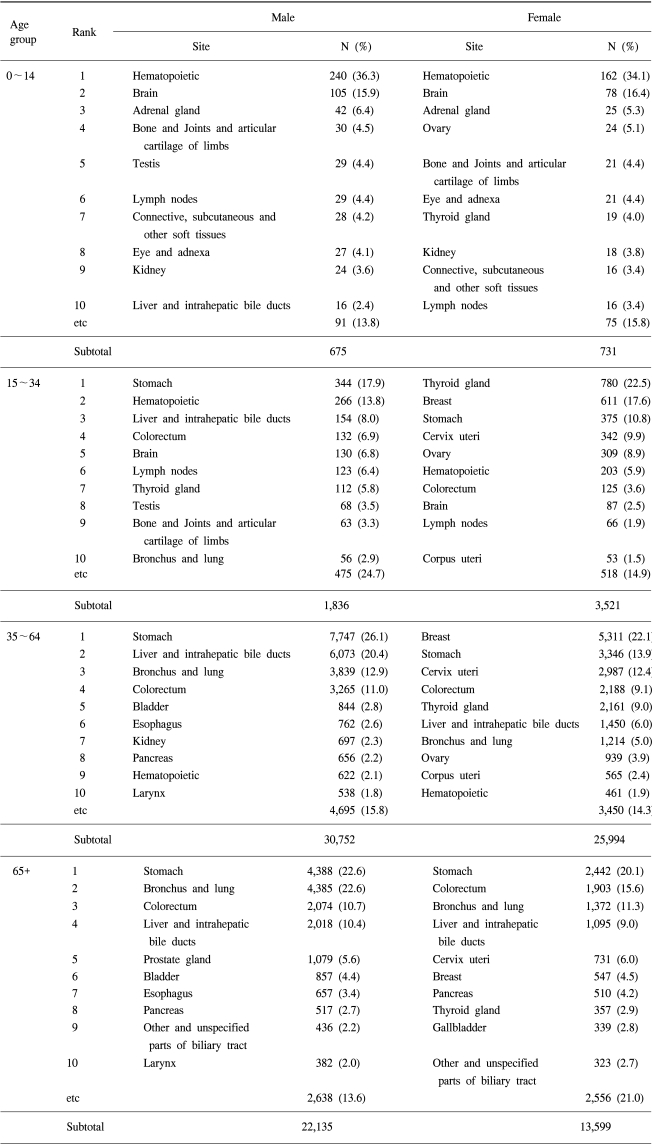
The most common cancer among children (0~14 years old) was in the hematopoietic & reticuloendothelial systems, with 36.3% of boys and 34.1% of girls. For the age group 15~34, stomach cancer was the most common cancer among males (17.9%) and thyroid cancer among females (22.5%). For the males in the older age groups, the stomach was leading site of cancer, at 26.1% and 22.6% among 35~64 year olds and those 65 and over, respectively. However, among the females aged 35~64, breast cancer was the most common cancer (22.1%), with stomach cancer being the most common among those 65 and over (20.1%) (Table 2).
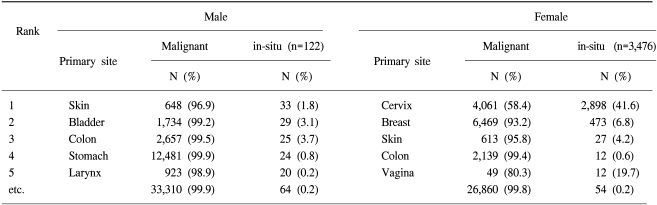
Table 3 shows the number of carcinoma in situ cases by gender. 41.6% of registered uterine cervix cases were carcinomas in situ. However, only 6.8% of registered female breast cancer cases were diagnosed as carcinomas in situ.
2) Distribution of the six major cancers by topographic and morphologic type
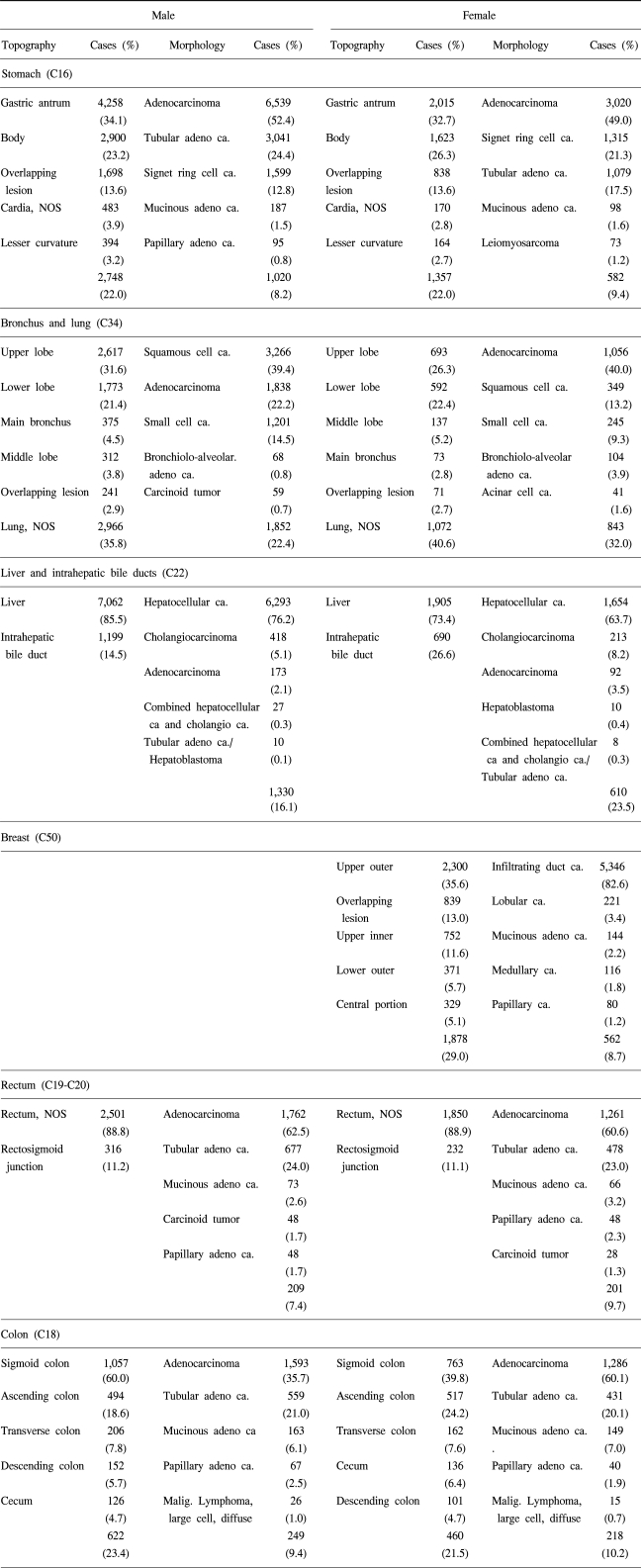
Table 4 shows the primary sites and morphologic types of the six major cancers by gender.
More than one third of stomach cancer (C16) occurred in the antrum part of the stomach (34.1% in males and 32.7% in females, respectively), and half of these were adenocarcinomas (52.4% in males and 49.0% in females). For bronchus and lung cancers (C34), the major primary site was the upper lobe (31.6% in males and 26.3% in females), with squamous cell carcinomas (39.4%) the major morphologic type in males, but adenocarcinomas (40.0%) in females. In males, hepatocellular carcinomas accounted for 76.2% of the liver and intrahepatic bile ducts cancers (C22); however, in females this was 63.7%. For breast cancer, 35.6% of female breast cancer (C50) occurred in the upper outer part of the breast, with 82.6% being infiltrating duct carcinomas. The most common site of colon cancer (C18) was the sigmoid colon (39.8% in males and 35.7% in females, respectively) and the most frequent morphologic type was adenocarcinomas (60.0% in males and 60.1% in females). Only 11.2% of male and 11.1% of female rectal cancers occurred in the rectosigmoid junction. As with other cancers, adenocarcinomas were the major morphologic type of rectal cancer (62.5% in males and 60.6% in females).
Appendix 2 shows the distribution of cancer cases by ICD-10 for easy comparison of the cancer death statistics.
DISCUSSION
Information on the incidence and mortality of cancers, and their changing trends, is an essential component in the planning and monitoring of programs for cancer prevention, early detection and treatment (2).
The Korea Central Cancer Registry (KCCR) was started as an ambitious project of the Ministry of Health and Welfare in 1980. In the beginning, 47 nationwide resident-training general hospitals participated in this program. The number of participating hospitals and registered malignancies has increased year-by-year, with 134 hospitals submitting their data diskettes in 2001 (1). The number of cancer cases in the KCCR for 2000 was assumed to be more than 90% precise for cancer cases, with the comparison of the estimated cancer incidence cases (3), using national mortality data, and the incidence data from four frontier regional cancer registries, including Kangwha, Seoul, Busan and Daegu, in the Cancer Incidence in Five Continents (4).
The KCCR database is especially useful for showing the trend of cancer occurrence in Korea, as information on the changing trend of cancer incidence over time is an essential component in the planning and monitoring of programs for cancer prevention, early detection and treatment. Major cancers, including stomach, lung, liver, breast and colorectum, but with the exception of uterine cervix cancer, were increasing (data not shown). For uterine cervix cancer, the proportion of carcinoma in-situ cases increased among the registered cases, meaning significant uterine cervix cancers were detected at an early stage.
Currently, KCCR, being a nationwide hospital-based cancer registry, is supporting technically and financially 9 population-based regional registries; Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, Ulsan, Jejudo and Goyang-si in 2003.
The KCCR database continues to hold the most important position until a nationwide, population-based data acquisition program can be constructed on the basis of international standards.
One area for caution in the interpretation of the KCCR data is that the numbers outlined in this report do not represent persons, but cases that have been reported. The patients who had cancers at several sites have been treated as multiple primary patients, and have been reported according to the cancer site.

 XML Download
XML Download