

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
More than 50% of patients with colorectal cancer have an incurable disease at the time of diagnosis, and are indicated for chemotherapy. Oxaliplatin and irinotecan, two newly developed agents with significant activity against colorectal cancer, have achieved relatively high response rates, but the median survival time has usually ranged from 9 to 12 months in patients who relapse following previous treatment with 5-FU and leucovorin (1). These results emphasize the need for new drugs and novel approaches in the treatment of metastatic colorectal cancer.
Chronotherapy consists of chemotherapy delivery according to biological rhythms along a 24-hour scale (2~6). These genetically based rhythms modulate the cellular metabolism and proliferation in normal tissues (7). As a result of chronotherapy, the tolerability and antitumor efficacy of 5-FU and oxaliplatin, among 30 anticancer drugs tested in laboratory rodents, varied largely according to the dosing time (8). Our aim was to transfer this concept to the clinic to primarily increase the dose-intensity. Specific technology (programmable-in-time injectors) allows for the administration of chronotherapy to fully ambulatory patients. Boughattas et al. administered lethal dose of oxaliplatin to 204 mice in one of three circadian stages (0, 8 or 16 hours after light onset), and found the toxicity was less severe at 16 hours (8). These results showed that administration of oxaliplatin during the daytime, especially 16:00 p.m., decreased the toxicities. The activity of dehydropyrimidine dehydrogenase increased around midnight and the tolerance of 5-FU is improved from 00:00 hours to 04:00 hours (9,10).
Fluorouracil (5-FU) has only achieved 10% of the objective responses in colorectal cancer, when given as a single agent for the first-line treatment of a metastatic disease (11). The objective response rate was increased by combining 5-FU with leucovorin (LV), as biochemical modulators (11,12), or by administrating 5-FU as a continuous venous infusion (11,13,14).
Oxaliplatin is a diaminocyclohexane platinum complex. Similarly to cisplatin and carboplatin, its main mechanism of action is mediated by the formation of DNA adducts. Oxaliplatin displays in vitro activity against human colorectal cancer cells (15), and has exhibited in vivo synergistic antitumor activity with 5-FU against transplantable tumor models (16,17). When used as a single agent, oxaliplatin achieved a 10~24% objective response rate in metastatic colorectal cancer (2,18~20).
The chronotherapy of oxaliplatin, 5-FU and leucovorin has achieved 51~67% objective responses and shown good tolerability in previously untreated metastatic colorectal cancer (3~6). In two phase III trials, chronotherapy reduced the toxicities and significantly increased the objective response rate (51~53%) compared with a constant-rate infusion of oxaliplatin (29~32%)(5,6).
Herein, the efficacy and toxicity of chronotherapy of oxaliplatin, 5-FU and leucovorin has been investigated in patients with advanced colorectal cancer.
MATERIALS AND METHODS
1) Eligibility and patient evaluation
Eligible patients had a histologically or cytologically confirmed adenocarcinoma of the colon or rectum, with relapsed or progressive disease patients, after 5-FU based chemotherapy, and metastatic lesions were included. Other eligibility criteria were measurable or evaluable lesions of tumor, an age between 18 and 75 years, a performance status by the ECOG scale, of grades 0 or 1, adequate organ function and a life expectancy of at least 3 months. Pretreated patients had received 5-FU based regimens as adjuvant or palliative treatments.
Pretreatment evaluation included: a complete medical history and physical examination, complete blood cell counts, chemistry profile, CEA measurement, urine analysis, chest X-ray, and CT scans of the abdomen, pelvis and/or chest. A complete blood cell count was obtained before the start of each treatment cycle, together with a serum chemistry profile, CEA measurement, chest X-ray, physical examination and toxicity assessment. Patients had radiological tumor parameter assessments every two cycles. The tumor response classification was derived from standard WHO criteria: (1) complete response, complete disappearance of all symptoms and signs of disease for a minimum of 4 weeks; (2) partial response, a 50% reduction (or more) in the sum of the products of the perpendicular diameters of measurable disease and the appearance of no new malignant lesion for a minimum of 4 weeks; (3) stable disease, no appearance of new areas of disease or less than 50% decrease or less than 25% increase in the described measurements; and (4) progressive disease, more than 25% increase in the measurements and/or appearance of new lesions. Patients who had evaluable lesions only were classified as having improved, stationary and progressive status according to the CEA and radiological imaging studies. The response based on the CEA assessment was defined as a morethan 50% drop in the serum CEA level for more than four weeks (21).
The toxicities of each course were recorded prior to the commencement of the subsequent course, and were graded according to the WHO criteria for neutropenia, anemia, thrombocytopenia, alopecia, nausea, vomiting, diarrhea, mucositis and peripheral sensory neuropathy.
2) Treatment
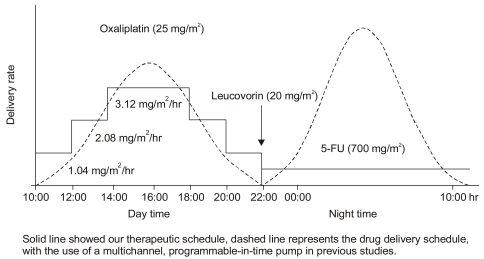
Patients received a 5-day course of chronomodulated, intravenously infused oxaliplatin (25 mg/m2/d), from 10:00 hours to 22:00 hours, with a continuous infusion of 5-FU (700 mg/m2/d) following a leucovorin bolus infusion (20 mg/m2/d) from 22:00 hours to 10:00 hours. This 5-day schedule (OHP-FL) was repeated every 3 weeks. Because a programmable-in-time, multichannel ambulatory pump for chronotherapy, with a sinusoidally varying delivery rate and peak delivery at 16:00 p.m., was not available, the authors modified the infusion rate using a stepladder configuration (Fig. 1).
Dose modifications were based on the complete blood cell counts taken the day before the next planned treatment. In case of grade 3 or 4 non-hematologic or grade 4 hematologic toxicities in the previous cycle, the oxaliplatin was reduced by 25% in the subsequent cycles, and the next course was delayed until complete recovery. The dose modification of 5-FU was performed as above.
RESULTS
1) Patients and treatment
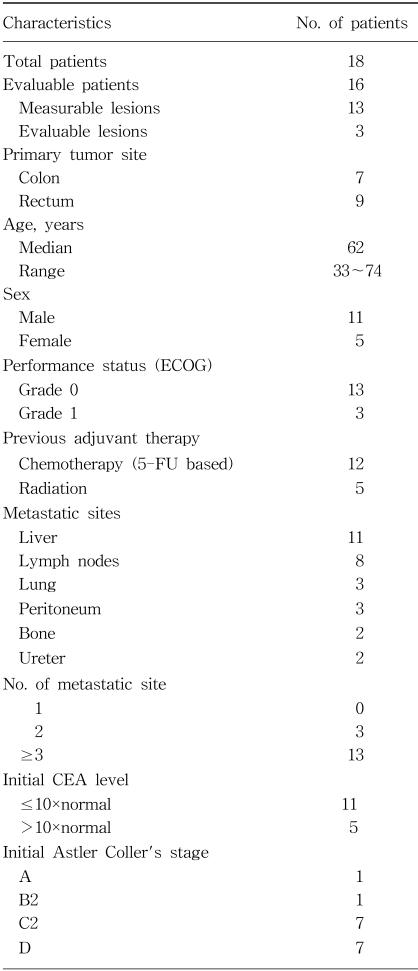
From March 1999 until December 2001, a total of 18 patients were enrolled. Two of these patients were excluded as they refused treatment after 1 cycle. Thirteen patients had measurable lesions and 3 did not, but all lesions were evaluable. Table 1 lists the demographic data, baseline disease and pretreatment characteristics for all patients. The median age of the patients was 62 years, ranging from 33 to 74. There were 11 male and 5 female patients. Seven and 9 patients had colon and rectal cancers, respectively. The most common disease sites were the liver (11 patients) and lymph node (8 patients).
Twelve patients had previously received chemotherapy containing 5-FU. Nine of the 12 previously-treated patients received chemotherapy as an adjuvant therapy. A relapse occurred after more than 6 months of adjuvant chemotherapy in 6 of these 9 patients. Fourteen patients had received surgery to remove the primary tumor, with 5 rectal cancer patients having received postoperative irradiation. Only 4 patients received OHP-FL chronotherapy as a first-line therapy with no other chemotherapy or radiotherapy. Of the 7 patients with colon cancer, 6 received a curative or palliative resection, and 4 received adjuvant chemotherapy. Of the 9 patients with rectal cancer, 8 received surgery, 5 of whom received adjuvant radiotherapy and chemotherapy, including 5-FU.
A total of 81 cycles of OHP-FL chemotherapy were performed (median: 5.5 cycles, range: 3~6 cycles). Two patients with ureteral metastasis had good renal function and did not required reduce chemotherapy. The mean dose-intensity (DI) of oxaliplatin per course was 34.8 mg/m2/week/course, which was 16.5% lower than that initially planned. The mean DI of 5-FU per course was 916.2 mg/m2/week/course, which was 22.5% lower than that initially planned. The median interval between the first days of two consecutive courses was 23 days (range, 19~36 days). Treatment was delayed for a median of 7 days for 18 (22%) of the eighty-one cycles.
2) Antitumor efficacy
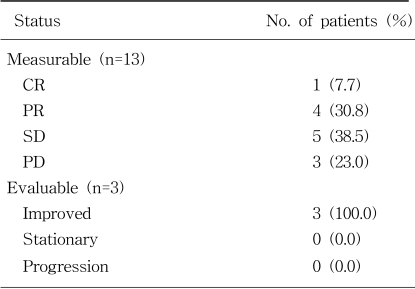
The response rate was 38.5% (95% confidence interval [CI], 13.9% to 68.4%) for the 13 measurable patients, including 1 CR (7.7%) and 4 PR (30.8%). Five (38.5%) had stable disease and 3 (23.0%) progressive disease (Table 2). The response rate by intent-to-treatment was 33.4%, including 6.7% CR and 26.7% PR. Of the 4 patients who received OHP-FL chronotherapy as the first-line chemotherapy, without previous 5-FU based chemotherapy or radiotherapy, 3 showed a PR and the other a progressive disease. Of the 12 patients previously treated with 5-FU based chemotherapy, 1 showed CR, 1 PR, 5 stable disease (SD), 2 progressive disease (PD) and 3 improved status. Of the nine relapsed patients after the adjuvant chemotherapy 1 showed PR, 5 SD, 1 PD and 2 improved status. The three patients without a measurable lesion had an improved status. The serum CEA level was observed to drop morethan 50% and the small peritoneal lymph nodes (less than 1 cm) were decreased in all 3 patients.
Two patients showed complete disappearance of liver metastasis after the OHP-FL chronotherapy. One patient was assessed as CR who had initially been diagnosed as Astler-Coller stage D of rectosigmoid cancer, with multiple metastatic liver masses. He had received radiotherapy and chemotherapy with 5-FU and leucovorin, and then palliative surgery for resection of the primary rectosigmoid cancer due to obstruction symptoms. After 6 cycles of OHP-FL chronotherapy, the metastatic liver masses had all disappeared on the serial follow up CT finding, but had progressed 29 weeks later. Another rectal cancer patient, assessed as PR, with 3 metastatic masses in the liver, had received 4 cycles of OHP-FL chronotherapy. The metastatic masses of the liver completely disappeared. He received surgery for resection of the primary rectal cancer, with the result of the pathology revealing stage B2, with no recurrence until recently.
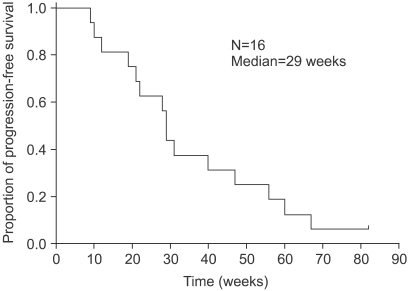
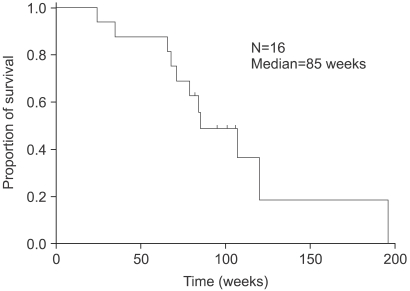
The median follow-up duration, time to progression (TTP) and overall survival were 85 (range, 24.0~196.0 weeks), 29 (Fig. 2) and 85 weeks (Fig. 3), respectively. The TTP and overall survival between the first- and second-line OHP-FL chemotherapy was not significantly different (p=0.45, p=0.61). With 2 subgroups of second-line OHP-FL chemotherapy, the TTP and overall survival of relapsed patients, compared with those of metastatic patients, were not statistically different (p=0.30, p=0.18). The survival rate of liver metastasis with lymph node involvement, compared with that of other metastatic sites, was not statistically different (p=0.10). Of the 16 patients, 11 died.
3) Toxicities
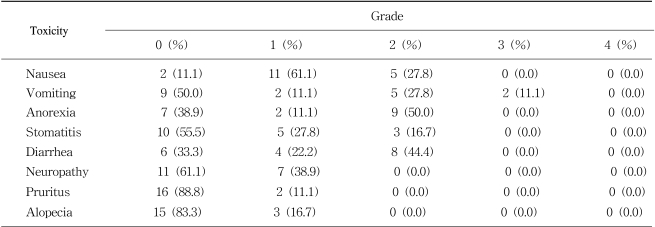
The incidences of hematological and non-hematological toxicities are summarized in Tables 3 and 4, respectively. There was 2.5% grade 3 thrombocytopenia (2 cycles), and 11.1% of grade 3 vomiting (2 patients). Anorexia, stomatitis, diarrhea, pruritus, alopecia and peripheral neuropathy were mild and tolerable (Table 4). No treatment-related mortality, infection and neutropenic fever occurred. No hand-foot syndrome developed.
DISCUSSION
The results of this study have shown that the efficacy of a chronomodulated infusion of oxaliplatin, 5-FU and leucovorin are comparable with the constant-rate infusion, FOLFOX regimen. The response rate was 38.5% (1 CR and 4 PR), and 1 of partial responders who had rectal cancer with 3 metastatic masses in the liver, who had received 4 cycles of chemotherapy. The metastatic masses of the liver completely disappeared. He received surgery for resection of the primary rectal cancer, with the pathology results revealing stage B2. FOLFOX studies have shown relatively lower response rates, of between 20 and 36%, with the exception of FOLFOX2 (46%)(22~25).
The role of chronotherapy has been investigated in several trials. In phase II trials, a chronomodulated infusion of oxaliplatin achieved a relatively high objective response rate (58~67%) and complete response rate (3~11%), with good tolerability in patients previously untreated for metastatic colorectal cancer (3,4). In phase III trials, chronotherapy reduced the incidences of severe toxicities (grade 3 or 4), while significantly increasing the objective response rate (51~53%) compared with the constant-rate delivery oxaliplatin schedules (29~32%)(5,6).
In this study, the objective response rate was lower than those of previous trials. One of the possible explanations is that all 3 drugs were chronomodulately infused in these trials, while only the oxaliplatin was chronomodulately infused in this study. A second could be the small size of enrolled patients, as this study was only a pilot. A third explanation could be that the patients in this study had more advanced stages, with 2 or more metastatic sites, than those in previous studies, with those enrolled almost receiving the treatment as a second-line chemotherapy.
In this trial, the oxaliplatin was infused step by step, with a peak delivery rate at 16:00 hours, with the 5-FU infused at a constant rate overnight (Fig. 1). This schedule was devised to avoid using the programmable-in-time injectors, with the convenience of an overnight infusion. Most chronomodulated infusion trials have been designed to infuse 5-FU from 22:00 hours to 10:00 hours, with a peak delivery rate at 04:00, with oxaliplatin from 10:00 hours to 22:00 with the peak delivery rate at 16:00 hours (3~6). Our modified infusion schedule may affect the efficacy and toxicity of this three-drug regimen.
Besides the efficacy, the toxicity of this regimen was tolerable. There was 2.5% grade 3 thrombocytopenia (2 cycles), and 11.1% grade 3 vomiting (2 patients). In previous chronomodulated infusion trials, grade 3 or 4 neutropenia occurred with 0.1~1.8% of the courses, and grade 3 or 4 thrombocytopenia with 0.1~0.4% of the courses (3,4). Grade 3 or 4 nausea and vomiting occurred in 24~37.8% of patients (4~6). Grade 3 or 4 diarrhea did not occur in our study, but frequently occurred in 24~41% of the patients in previous trials (4~6).
Peripheral sensory neuropathy was the cumulative dose-limiting toxicity. Seven patients complained of grade 1 neurotoxicity. In previous trials, grade 2 peripheral sensory neuropathy occurred in 25.6~27% of the patients, but no grade 3 or 4 neuropathy occurred (4,5). In another report, grade 1 or 2 neuropathy occurred in 453 courses (58%), while grade 3 or 4 neuropathy occurred in 86 courses (11%), which eventually led to oxaliplatin withdrawal in 14 patients after 7~12 courses, with complete recovery within 3 months (3).

 XML Download
XML Download