

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Colorectal cancer is the 4th most common cancer in Korean both men and women (1). Although surgery is potentially curative, about 50% of all newly diagnosed patients will ultimately develop an incurable metastatic disease, even if adjuvant treatment is used (2). 5-Fluorouracil (5-FU) based chemotherapy has been demonstrated to prolong survival and to improve the quality of life in patients with metastatic colorectal cancer (3). New agents, such as irinotecan and oxaliplatin, have also demonstrated antitumor activity in this disease. Therefore, chemotherapy of metastatic colorectal cancer has profoundly changed in the past few years, moving from a fluoropyrimidine-modulated treatment to a more aggressive approach that includes two active agents (4).
Oxaliplatin has a mechanism of action similar to that of other platinum derivatives, although its spectrum of antitumor activity against tumor models differs from those of cisplatin and carboplatin. Activity against cisplatin-resistant colon carcinoma cell lines has been demonstrated (5). The toxicity of oxaliplatin is also distinct from other platinum drugs: it has no renal toxicity and minimal hematotoxicity; it causes both a reversible acute, cold-related dysesthesia and a dose-limiting cumulative peripheral sensory neuropathy, which usually rapidly regresses after treatment withdrawal. The activity of a single agent in metastatic colorectal cancer patients either previously untreated or treated with 5-FU was demonstrated in phase II trials, with response rates ranging between 10% and 24% (6,7). Consistent with laboratory evidence of oxaliplatin/5-FU synergy, there is evidence for the clinical activity of 5-FU plus leucovorin (LV) and oxaliplatin combinations, with reported response rates of ranging from 20% to more than 50% reported for the three-drug combination in phase II trials (8,9), although the optimal regimen has yet to be determined.
We previously reported on the efficacy of oxaliplatin with the Mayo Clinic regimen in 5-FU refractory colorectal cancer (10). However, that regimen had a relatively higher toxicity than in previous studies, so we used a modified FOLFOX 4 regimen, which comprised of a simplified biweekly low dose LV, 5-FU combined with oxaliplatin as a first line therapy for patients with colorectal cancer. The primary objective of this study was to assess the efficacy, and response rate and the feasibility of this regimen: the secondary objectives included the evaluation of toxicity, progression free survival, and overall survival in patients with metastatic progressive colorectal cancer.
MATERIALS AND METHODS
1) Eligibility criteria
Patients were required to have a histologically confirmed adenocarcinoma arising in the colon or rectum and radiographical evidence of a metastatic disease. Patients who had previous adjuvant chemotherapy were eligible if they had completed treatment more than 6 months before registration in this study. All patients had bidimensionally measurable lesions ,and, a performance status less than or equal to 2 according to the ECOG scale, and had adequate bone marrow and renal function, and age between 18 and 75 years. Exclusion criteria included the presence of CNS metastases, serious or uncontrolled concurrent medical illness, and a history of other malignancies. Written informed consent was obtained from each patient prior to study entry.
2) Treatment protocols and dose modification
On day 1, oxaliplatin (85 mg/m2) was administered by intravenous (iv) infusion in 500 ml of normal saline or dextrose over 2 hours. On days 1 and 2, LV (20 mg/m2) was administered as an iv bolus, immediately followed by 5-FU (400 mg/m2) given as a 10 minute iv bolus, followed by 5-FU (600 mg/m2) as a continuous 22 hour infusion, with a light shield. Dose modifications of oxaliplatin or 5-FU were made for hematologic, gastrointestinal or neurologic toxicities on the basis of the most severe grade of toxicity that had occurred during the previous cycle. Treatment could be delayed for up to 2 weeks if symptomatic toxicity persisted, or if the absolute number of neutrophils was lower than 1,500/µl; platelets count was lower than 100,000/µl. The 5-FU dose was reduced by 25% for subsequent courses after National Cancer Institute common toxicity criteria (NCI-CTC) grade 3 diarrhea, stomatitis, or dermatitis had occurred. The dose of oxaliplatin was reduced by 25% in subsequent cycles if there was persistent paresthesias persistent between cycles or paresthesias with functional impairment lasting more than 7 days. Treatment was continued until there were signs of disease progression, unacceptable toxic effects developed, or the patient refused further treatment.
3) Pretreatment and follow up evaluation
Before the each treatment courses, a physical examination, routine hematology, biochemistry, and chest X-ray were performed. The serum CEA levels were determined after each cycles. CT scans to define the extent of the disease, and the responses were performed after 4 cycles of chemotherapy, or sooner if there was evidence of any clinical deterioration. Patients were assessed before starting each 2-week cycle using the NCI-CTC, except in the case of neurotoxicity. For the neurotoxicity, an oxaliplatin-specific scale was used: grade 1, paresthesias or dysesthesias of short duration, but resolving before the next dosing; grade 2, paresthesias persisting between doses (2 weeks); and grade 3, paresthesias interfering with function.
4) Assessment of response
The antitumor activity was evaluated according to the WHO criteria., and the dose-intensity (mg/m2/wk) was calculated as the total cumulative dose divided by the duration of dosing. The Rrelative dose-intensity (RDI) was calculated as the dose-intensity divided by the planned dose-intensity, multiplied by 100. The planned dose-intensities, expressed as milligrams per square meter per week, were 1,000 for 5-FU and 42.5 for oxaliplatin.
5) Statistical methods
The variables for inclusion in the model were gender, age, primary site of disease, number of metastasesis, previous adjuvant chemotherapy or radiation treatment, and the baseline CEA. The comparison of the response rates for the different variables was performed using the Fisher's exact test. The time to progression, and overall survival were calculated using the Kaplan-Meier method. The time to progression was calculated from the date therapy started to the date of disease progression, and the overall survival was calculated from the date therapy started to the date of death. Differences between the Kaplan-Meier survival curves were tested using the log-rank test. All data were analyzed using SPSS software (version 10.0).
RESULTS
1) Patient characteristics
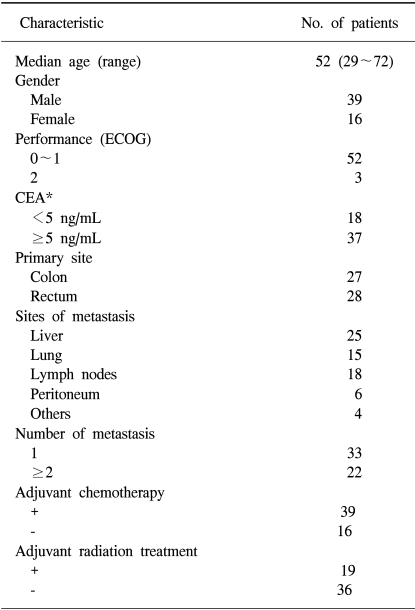
Between March 2001 and August 2003, a total of 55 patients were assigned to treatment at the department of Internal Medicine of Dong-A University Medical Center, Busan, Korea. Five patients were not evaluable for this study because of loss to follow up or than 2 cycles of chemotherapy, and 50 were evaluable for response and toxicity. The patient's characteristics are listed in Table 1.
2) Objective tumor responses and survival
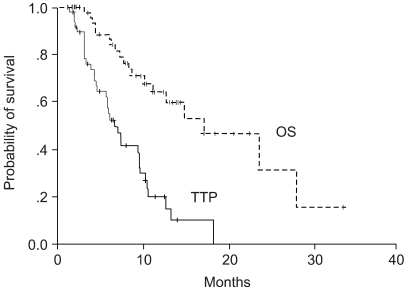
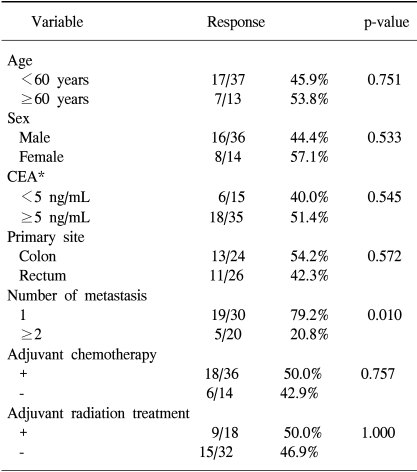
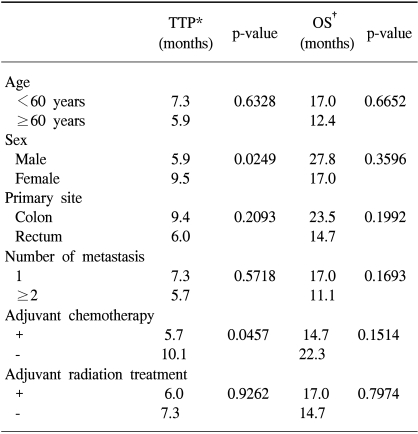
The response rate in the intent to treat population of all 55 patients was 40%. According to the per protocol analysis, the response rate was 44% (22/50). Three patients achieved a CR, 19 a patients achieved PR, 17 a patients SD, and 11 patients showed a progressive disease during the course of the treatment. Patient's age, gender, and CEA level before chemotherapy, and site of metastasis, number of metastasesis, adjuvant chemotherapy and adjuvant radiation therapy did not effect on the response rate. Patients who had a single metastasis were better responded better to the FOLFOX 4 regimen (Table 2). The median follow up duration, time to progression and overall survival were 10, 6.6 (95% CI: 4.98~8.02 months), and 17.0 months (95% CI 9.15~24.85 months), respectively (Fig. 1). A longer time to progression was observed in the female patients, and those with primary metastasis had a longer time to progression than relapsed patients, but there was no difference in the overall survival. At the time of this report, an irinotecan-based second-line regimen was administered into 25 patients (50%). The reason why female patients achieved a shorter overall survival, even though there was a significantly longer time to progression, may have been due to more male patients were responded to second line chemotherapy {20% (3/15) vs. 10% (1/10)}. There were no differences in the time to progression and overall survival among the other variables (Table 3).
3) Toxicity
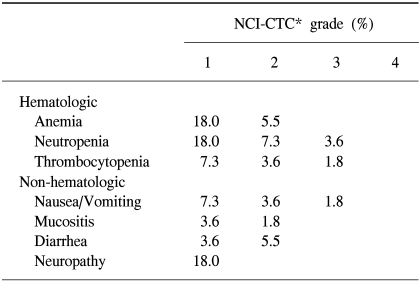
A total of 278 cycles of chemotherapy were administered to the 55 patients. The median number of cycles was six, ranging from 2 to 9 cycles. On the whole, the data indicate that this regimen was well tolerated throughout the study. The incidences of hematologic toxicities and non-hematologic toxicities weare summarized in Table 4. Febrile neutropenia requiring hospitalization and treatment with intravenous antibiotics developed in one patient at two cycles (0.7%). Peripheral neuropathy appeared in the forms of transient cold exacerbated paresthesia or dysesthesia. Three patients required dose reductions for acute hematologic toxicity, and another one patient required eventual dose reduction throughout the course of therapy due to grade 3 nausea/vomiting. The relative dose intensitiesy of oxaliplatin and 5-FU were 95.4% and 92.6% of the projected doses. There was no treatment related death.
DISCUSSION
During the past 3 years, multiagent chemotherapy, consisting of either irinotecan or oxaliplatin combined with fluorouracil and leucovorin, has largely supplanted 5-FU based chemotherapy as the first-line treatment for metastatic colorectal cancer. This shift occurred as a result of randomized, controlled trials demonstrating significant improvements in objective response rates, time-to-tumor progression,; and, for irinotecan, survival using multiagent chemotherapy (11,12).
Two randomized studies from Europe reported promising results with oxaliplatin, 5-FU, and LV as a first-line treatment compared with 5-FU and LV alone (12,13). Both studies showed significantly better response rates and progression-free survival by the addition of oxaliplatin, but with no improvement in the overall survival. The lack of an overall survival benefit might be partly explained by the high proportion of patients who crossed over to oxaliplatin or received irinotecan as second-line treatment. The United States Intergroup study N9741 used IFL (Iriontecan/5-FU/LV) as the control arm of the study and compared it with oxaliplatin and infused 5-FU/LV (FOLFOX4) or irinotecan/oxaliplatin in the first-line treatment of colorectal cancer. FOLFOX4, compared with IFL, produced a better overall survival (median, 19.1 vs. 14.8 months, respectively; p=.006), time to disease progression (median, 8.8 vs. 6.9 months, respectively; p=.004), and response rate (40% vs. 30%, respectively; p=.02), but the overall quality of life data wereas similar (14).
Although it is clear that both oxaliplatin and 5-FU are required to obtain the beneficial effects of this therapy, oxaliplatin has also been evaluated in combination with 5-FU using several alternative administration methods. These have included short-term (24- or 46-hour) or long-term (continuous) infusions of 5-FU (with or without the bolus 5-FU component), a daily or weekly bolus 5-FU bolus, without the infusional component (15), or substitution for FU with the oral FU prodrug, capecitabine (16).
The FOLFOX4 regimen, combining oxaliplatin with LV5FU2, represented the most extensively studied oxaliplatin-containing regimen, with consistently high levels of antitumor activity against colorectal cancer in phase III clinical trials (12,14). Despite the benefits seen with FOLFOX4, the infusion schedule used in FOLFOX4 is cumbersome and requires frequent hospital or clinic visits. Simplified infusion schedules of FU/LV have been developed with similar efficaciesy (17). The combination of oxaliplatin and capecitabine has been used as a first-line therapy, with overall response rates of 43% to 55%, a progression-free survival time of 6 to 7.6 months, and a median overall survival time of 17.1 to 19.5 months (16,18). The results obtained in these studies were comparable with those achieved with FOLFOX 4. Randomized trials are being planned to compare oxaliplatin and capecitabine, with FOLFOX4, in both the first- and second-line settings.
A French group compared the single-agent thymidylate synthase inhibitor, raltitrexed, with 3 different 5-FU infusion 5FU schedules in first-line metastatic colorectal cancer (19). Given the various 5-FU infusion regimens, a standard de Gramont schedule of 5-FU following a 200 mg intravenous infusion of LV over 2 hours (LV5FU2) vs. a low-dose 20 mg intravenous bolus of LV (ldLV5FU2) were used. The third infusion 5-FU arm employed a modified AIO (German Association of Medical Oncology) dose of 2.6 g/m2 of 5-FU infused over 24 hours every week for 6 weeks in a 56-day cycle (HD-5FU). The authors concluded that ldLV5FU2 was an active, easier and less expensive schedule of infusional 5-FU than the classical LV5FU2 or weekly HD-5FU. In this study, low dose LV was used, but showed no influence on the overall outcome of the de Gramont infusion regimen.
The toxicity and tolerability profiles of the regimens evaluated in this study were similar in scope, and frequency, but with lower intensitiesy to those reported by others authors (12,14). In this phase II study, performed at a single institution, we found the toxicity profile was found to be highly acceptable, with a lower rates of hematologic toxicity and gastrointestinal toxicitiesy. Neurotoxicity was the principal toxicity and dose limiting toxicity of oxaliplatin, with two distinct syndromes, acute neurosensory toxicity, characterized by paresthesias and dysesthesias occurring shortly after infusion, and long-term toxicity, characterized by a sensory neuropathy that occurrings with chronic dosing of oxaliplatin (20). On cessation of the drug, the chronic neurotoxicities improved in the majority of patients within 4 to 6 months, and were completely resolve in approximately 40% of patients by 6 to 8 months (21). The likelihood of symptomatic improvement on discontinuation of oxaliplatin correlates inversely correlated with the cumulative dose. Several strategies to decrease the incidence of peripheral neurotoxicity have been evaluated, such as the use of carbamazepine, gabapentin, calcium/magnesium infusions, and glutathione (21,22). Severe peripheral sensory neuropathy (grade 3 to 4) normally occurs in 10% to 15% of patients after a cumulative dose of 780 to 850 mg/m2 of oxaliplatin (21). In this study, the median number of oxaliplatin courses was six, giving a cumulative dose of 510 mg/m2. This may explain the low incidence of severe peripheral neuropathy.
The emergence of irinotecan and oxaliplatin as key components of multidrug chemotherapy for colorectal cancer has challenged our ability to integrate both of these new agents into therapeutic regimens in a rational, yet expeditious fashion. An Italian group reported promising result with a three drug regimen (biweekly chemotherapy with oxaliplatin, irinotecan, infusional fluorouracil and leucovorin (23). It may be impossible to know whether it is better to administer these drugs in a simultaneous or a sequential fashion without performing a phase III trial. However, even before this can be carried out, the therapeutic options for advanced colorectal cancer are likely to change with the addition of cetuximab, and bevacizumab (24,25).
 XML Download
XML Download