

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Inedible foreign body (FB) ingestions occur more frequently in denture users, incarcerated individuals, and patients with psychiatric disorders or alcohol intoxication.1
Before the double-balloon enteroscopy (DBE) era, daily radiographs were recommended to ensure the safe passage of a FB through the small bowel. If there is no distal progression over a 3-day period or if the patient becomes symptomatic, emergency surgical consultation should be obtained.2 DBE has led to improvements in both the diagnosis and therapy of small bowel bleeding. DBE is also reported to be clinically useful for management of small bowel Crohn's disease and tumors.34
In cases of FBs in the small bowel, conservative management may be inappropriate in a patient with autism because of an inability to properly assess the symptoms. A sharp-oriented FB in the small bowel has a high risk of intestinal perforation.1 DBE is expected to be useful clinically for removal of sharp FBs beyond the reach of conventional endoscopy.
CASE REPORT
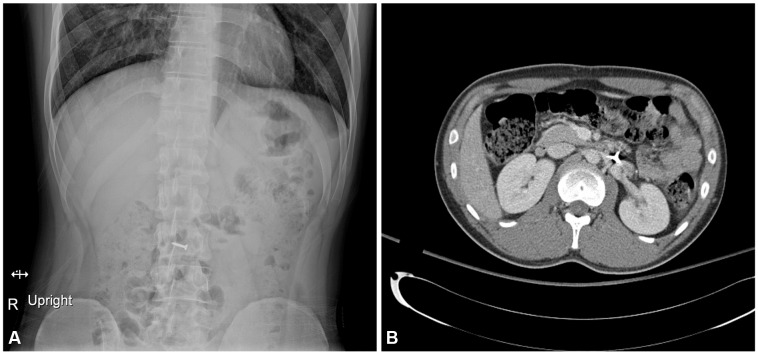
A 19-year-old male patient with autism was referred to our hospital because of suspected ingestion of a FB. His teacher found that a 1.5-cm sharp-oriented screw nail was missing from his table in the crafts class of a special school for the disabled, and his teacher suspected that he had ingested it 3 hours before referral. He did not present any symptoms. He did not have a previous history of pica. We were unable to obtain the patient's history and perform a physical examination due to the patient's noncooperation and intellectual disability. His laboratory examination showed leukocytosis (13,200/µL); other values were unremarkable. Abdominal simple radiography detected the presence of foreign material (Fig. 1A). Abdominal computed tomography facilitated determination of the location of the FB and revealed a sharp, pointed screw nail in the proximal jejunum without evidence of small bowel perforation (Fig. 1B). We decided to remove the FB endoscopically because of its sharp nature and difficulty in the assessment of the patient's symptoms. The procedure was performed using the 9.5-mm enteroscope Fujinon EN-450T5 (Fujinon Inc., Saitama, Japan). The examination began with the overtube back-loaded onto the endoscope with both balloons collapsed. The endoscope was advanced into the bowel lumen until no further advancement was possible. The balloon on the tip of the endoscope was then inflated. This was followed by inserting the overtube into the lumen and inflating the overtube balloon. Using the overtube as an anchor, the balloon of the endoscope was deflated, and the endoscope was advanced deeper into the small bowel. Thus, the endoscope was advanced along the small bowel by inflating and deflating the two balloons.
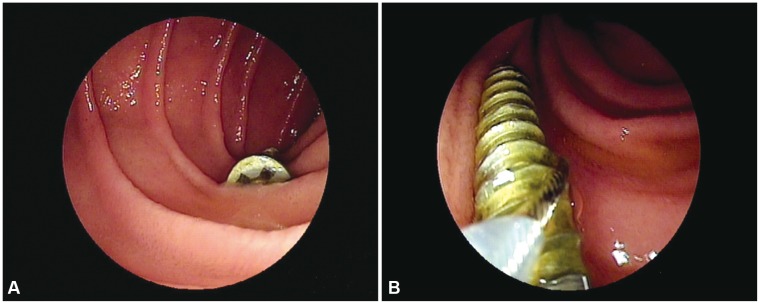
The oral approach was determined based on the assumed location of the FB. Sedation was achieved using midazolam (10 mg) and meperidine (50 mg). The patient was 177 centimeters tall and weighed 73 kg. Initially, doses of midazolam 3 mg and meperidine 50 mg were administered to him. During the endoscopic procedure, the oxygen desaturation was not seen but he was not calmed down and uncooperative with initial administration of combined midazolam and meperidine. Consequently, we restrained him and injected additional dose of midazolam. Therefore he was administered midazolam additionally up to total dose of 10 mg for proper conscious sedatation. DBE revealed that the FB was located in the proximal jejunum; no endoscopic evidence of perforation was identified (Fig. 2A).
Endoscopic removal of the screw nail was attempted using a polypectomy snare. Initially, we tried to hold the sharp end of the screw nail and push and pull the scope backwards towards the oral side, hoping not to penetrate the jejunal wall and to avoid bending the snare arm (Fig. 2B). Finally, we released the screw nail from the jejunal wall, directing sharp end of the screw nail to the oral side, and removed it from the jejunum without complications. No complications were evident the day after the procedure, and the patient was discharged.
DISCUSSION
The management strategy for ingested FBs depends on their nature, location, duration of impact, and the patient's clinical status.1 If the FB passes into the stomach, endoscopic removal is needed in the following cases: a sharp FB, those longer than 6 cm in length or 2.5 cm in diameter, FB retention in the stomach beyond 3 to 4 weeks, battery retention in the stomach beyond 2 days, and magnets in the upper GI tract within the reach of endoscopy.7 Less than 1% of FBs that enter the stomach cause perforation of the bowel. However, the rate of intestinal perforation caused by sharp objects is reported to be 35% (usually at the ileocecal valve).1 Daily radiographs are recommended in cases of a sharp FB in the small bowel, even if the patient is asymptomatic. Unless there is distal progression over a 3-day period or if the patient becomes symptomatic, emergent surgical consultation had to be obtained.2
Before the era of DBE, X-ray photographs of the daily, has been recommended to ensure the safe passage of the FB in the small intestine. The rationale of "spontaneous passage" as a reason for the performance of daily radiographs mentioned in other reports likely accounts for the inability in the past to access conventional endoscopy. Therefore, enteroscopic removal may be justified in cases of sharp FBs in the small bowel.
Accurate assessment of the patient's clinical status is an essential prerequisite for conservative management of a sharp FB in the small bowel. If there is considerable concern in the assessment due to a developmental disorder such as autism, enteroscopic removal should be attempted when DBE is available for those cases of a sharp FB in the small bowel.
The DBE approach (oral versus anal) depends on the location of the ingested FB. CT is helpful for determining the location, as well as the size and shape, of a small bowel FB.8 In our case, the position of the screw nail was thought to be located 20 to 30 cm distal to Trietz ligament. It might have been successfully removed at this location using pediatric colonoscope. We decided to perform double balloon enteroscopy by fear for its more distal movement. That is because the endoscopic procedure or the physiologic peristalsis of small bowel might advance it toward the anal side.
Retrieval devices commonly used for a FB in the esophagus or stomach include rat-tooth and alligator forceps, polypectomy snares, baskets, and nets. Selection of these devices depends on the shape of the FB. For example, a net is most appropriate for the retrieval of coins or disc batteries. In the case of a sharp-oriented FB, a polypectomy snare is useful clinically.7 DBE (EN-450T5) is equipped with a 2.8-mm forceps channel that allows the use of almost all general therapeutic accessories. In the present case, the screw nail was easily captured by the polypectomy snare because of the spiral grooves present in the sharp-pointed portion.
When we remove a sharp-point object using snare, it might be safer to direct the sharp portion toward the oral side. However, we had a difficulty in facing its sharp portion toward the oral side. We carefully removed the nail by capturing its helical ridge being toward anal side. Fortunately, any complications such as laceration or perforation were not occurred.
In conclusion, this case adds to the growing body of evidence for the value of therapeutic DBE for removal of ingested FB in the small bowel.
 XML Download
XML Download