

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Patients with a Roux-en-Y anastomosis may present with various pancreaticobiliary problems requiring endoscopic intervention.1 However, performing endoscopic retrograde cholangiopancreatography (ERCP) in these cases is very difficult because conventional endoscopes can barely reach the papilla in the long afferent limb. Recent studies have suggested that balloon-assisted enteroscopy (BAE) can provide direct access to the major papilla in the afferent loop, and can therefore be used for ERCP in patients with a Roux-en-Y anastomosis.12 We experienced six cases involving Roux-en-Y anastomosis and biliary problems at our center, and assessed the utility of ERCP with single balloon enteroscopy (SBE) in these patients.
CASE REPORTS
A single balloon enteroscope with a length of 200 cm, distal end diameter of 9.2 mm, and channel diameter of 2.8 mm (SIF-Q260; Olympus Co., Tokyo, Japan) and an overtube (ST-SB1; Olympus Co.) were used to access the afferent limb in all cases. Because a routine ERCP catheter could not reach the ampulla using SBE owing to long channel length and a long ERCP catheter was not available in Korea, a self-assembled long catheter was used to acquire a cholangiogram in the first case. Single balloon enteroscope insertion followed by replacement with a conventional endoscope, as described previously,3 was used for ERCP in the next five cases because long accessories were not available.
Case 1
A 66-year-old man was transferred with a diagnosis of biliary sepsis. Computed tomography (CT) revealed a dilatation of the common bile duct (CBD) and a swelling of the pancreas with peripancreatic infiltration. One year previously, he had undergone a total gastrectomy with Roux-en-Y anastomosis for gastric cancer. ERCP was performed using a forward-viewing esophagogastroduodenoscope, but the ampulla could not be reached. The following day, ERCP using SBE was attempted, and the papilla was successfully reached in 29 minutes. To produce a long catheter, after removing the injection needle from the colonoscopic injection catheter, the injection catheter end was conjoined with the infusion part of the ERCP catheter. Using this self-assembled long catheter, cholangiography was performed and showed mild dilation of the CBD and pancreatic duct, but no visible stone. Based on these findings, we assessed that the biliary stone had already been passed. To improve pancreatitis, a plastic stent (5 Fr, 3 cm, Cook Medical Inc., Bloomington, IN, USA) was inserted into the pancreatic duct. The patient was discharged without complications 4 days later.
Case 2
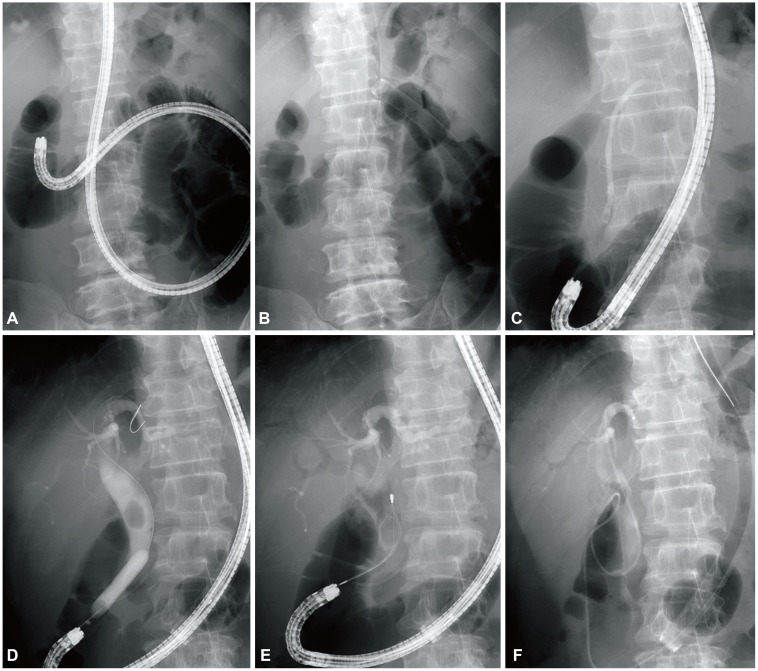
A 58-year-old man who had undergone a total gastrectomy with Roux-en-Y anastomosis for gastric cancer visited our emergency department with abdominal pain and fever. A CT scan revealed a 17-mm stone obstructing the CBD. A single balloon enteroscope was inserted, and the papilla was reached after 14 minutes. After shortening the small bowel, the enteroscope was withdrawn, leaving the overtube. An esophagogastroduodenoscope was successfully inserted through the in-dwelling overtube, and the standard accessories for ERCP could then be used. Cholangiography showed a diffuse dilatation and a 17-mm filling defect in the CBD. After dilating the papilla with a controlled radial expansion (CRE) balloon (Boston Scientific, Natick, MA, USA), a brown stone was removed using a mechanical lithotripter and retrieval balloon (Fig. 1). The patient experienced mild post-ERCP pancreatitis presenting with abdominal pain, a serum amylase level of 1,380 IU/L, and a serum lipase level of 2,969 IU/L, but recovered with conservative treatment. He was discharged 6 days after ERCP without event.
Case 3
A 73-year-old man who had undergone a total gastrectomy with Roux-en-Y anastomosis for gastric cancer was admitted for removal of a 12-mm CBD stone. Although the ampulla was reached using SBE in 38 minutes, the small bowel was not shortened effectively, and a conventional endoscope could therefore not pass through the overtube. The next best treatment option was to leave the guide wires in the afferent limb and introduce a pediatric colonoscope equipped with a cap along these wires, but this approach also failed. Consequently, percutaneous transhepatic choledochoscopy (PTCS) was performed.
Case 4
A 72-year-old woman visited the emergency department with epigastric pain and fever. A CT scan suggested CBD stones and cholangitis. Four years previously, she had undergone a total gastrectomy with Roux-en-Y anastomosis for gastric cancer. Jejunojejunostomy was performed by side-to-side anastomosis, and an extremely acute angulation was formed between the afferent and efferent limbs. Access to the papilla using SBE was therefore quite difficult, and 70 minutes were required. Replacing a conventional scope through the overtube was impossible owing to the angulation at the Roux-en-Y anastomosis. A CRE balloon was used at the collapsed site of the angulation, and the conventional scope was eventually passed. Although the conventional scope could reach the papilla, cannulation was not successful. Therefore, the CBD stones were removed by PTCS.
Case 5
A 69-year-old woman who had undergone a distal gastrectomy with Roux-en-Y anastomosis for gastric cancer visited the emergency room with abdominal pain, fever, and hypotension. A CT scan revealed calculous cholecystitis and a distal CBD stone. Percutaneous gallbladder drainage was performed initially, and SBE-assisted ERCP was attempted 2 days later. After accessing the papilla, the enteroscope was shortened and replaced with a pediatric colonoscope through the overtube. Cholangiography revealed a 12-mm filling defect. However, removal of the CBD stone failed because of poor maneuverability. The patient was eventually treated by percutaneous transhepatic papillary balloon dilation.
Case 6
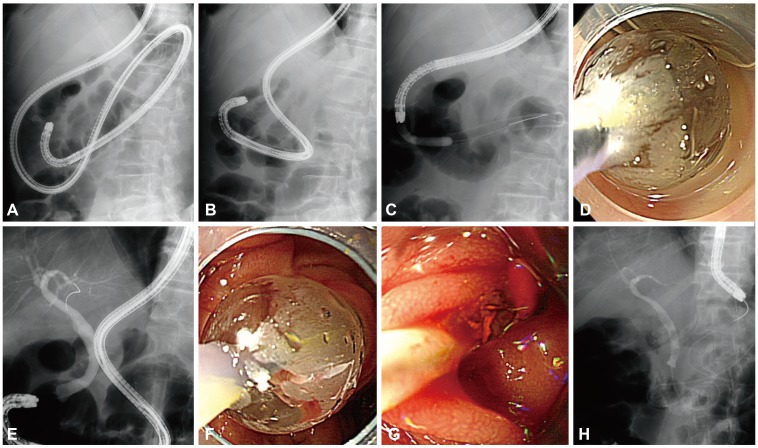
A 78-year-old man was transferred with a diagnosis of cholangitis. Three years prior, he had undergone a total gastrectomy with Roux-en-Y anastomosis for gastric cancer. A single balloon enteroscope was inserted into the afferent loop. After shortening of the small bowel, the enteroscope was retrieved, but the remaining overtube was collapsed because of the acute angulation of the small bowel. A CRE balloon was used to dilate the collapsed site, and a conventional endoscope could then be pushed into the overtube. Small brown stones were successfully removed by ERCP (Fig. 2).
DISCUSSION
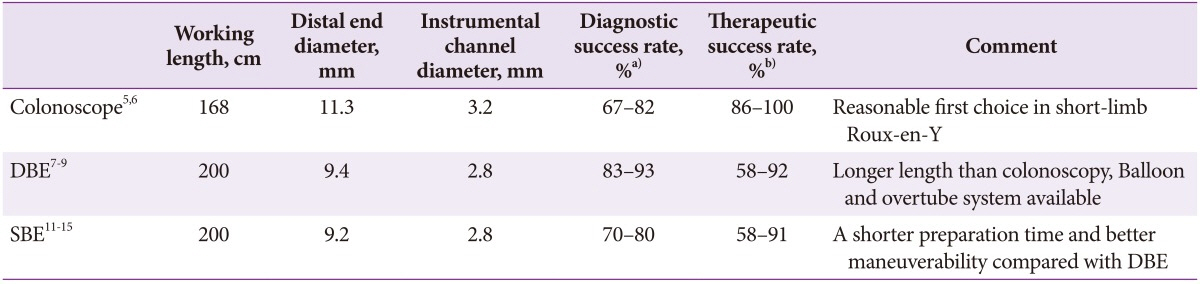
Patients who have undergone Roux-en-Y anastomosis sometimes present with pancreaticobiliary problems. Because ERCP in these patients is extremely difficult owing to their anatomical complexity, including a long afferent loop or difficulty in maneuvering, more invasive interventions such as percutaneous transhepatic biliary drainage, PTCS, or surgery are often necessary.4 ERCP using a forward-viewing endoscope such as a pediatric colonoscope might be the first choice treatment in patients with altered anatomy.56 BAE provides direct access to the major papilla located in the long afferent loop, and therefore, enables ERCP to be performed in patients who have had a Roux-en-Y anastomosis. ERCP using double balloon enteroscopy (DBE) is an innovative technique because of its ability to enable ERCP-related interventions in patients with altered anatomy after surgery.789 SBE has the advantages of a shorter preparation time and better maneuverability compared with DBE. ERCP using SBE was first reported in 2008,10 and several case series of SBE-ERCP in patients with Roux-en-Y anastomosis have been published.111213 Two studies that compared SBE-ERCP with forward-viewing endoscope (including colonoscope)-assisted ERCP14 or DBE-ERCP15 reported that SBE was not inferior in accessing the papilla or performing therapeutic ERCP in patients with a Roux-en-Y anastomosis. Table 1 showed the characteristics and diagnostic and therapeutic success rates of ERCP using colonoscopy, DBE, and SBE.
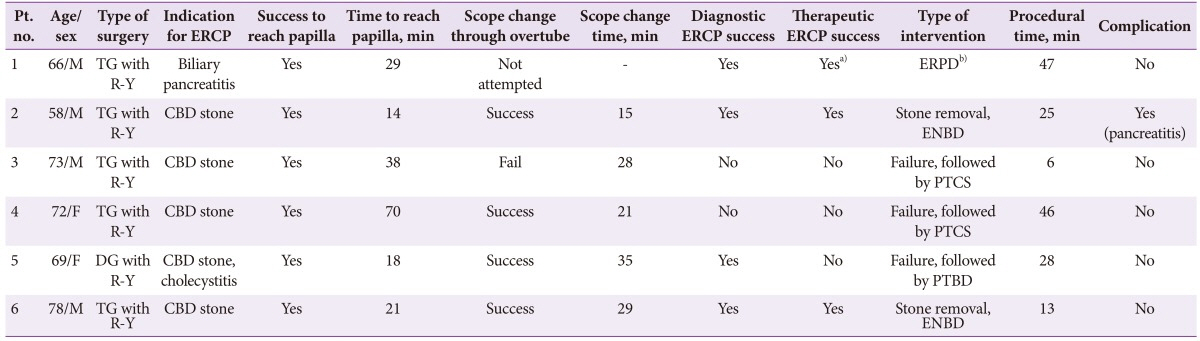
Based on the aforementioned studies, we attempted ERCP using SBE in patients with Roux-en-Y anastomosis due to biliary problems. Although the papilla was reached using SBE in all patients, a cholangiography that secured the diagnosis was obtained in four of six cases, and therapeutic intervention succeeded in only three (Table 2). Technical inexperience might have influenced this relatively low therapeutic success rate. The absence of an elevator in the enteroscope or conventional endoscope also limited maneuverability during ERCP. Because long accessories compatible with an enteroscope were not available, we chose to perform single balloon enteroscope insertion followed by replacement with a conventional endoscope, which enabled us to use standard accessories. Unlike the report of Itoi et al.3 that first described such an exchange method and a success rate of 72.1% (8/11) in patients with Roux-en-Y anastomosis, our success rate was relatively low. However, a direct comparison between the results of this study and those obtained in the study by Itoi et al.3 is not possible owing to differences in surgical methods, the degree of postoperative intra-abdominal adhesion, and the endoscopist's experience. To perform ERCP in patients with altered anatomy, various other methods including short type SBE,16 short type DBE,17 the endoscopic ultrasound-guided antegrade approach,18 and cap-assisted approach19 have been introduced with success rates ranging from 70% to 98.5%.
Complications such as bleeding, infection, and perforation can occur with ERCP using BAE owing to long procedure times and the level of difficulty involved. In our study, the mean procedural time was 80.5 minutes (range, 54 to 137). However, only one patient experienced mild pancreatitis after ERCP despite the relatively long procedure time. According to earlier reports on SBE-ERCP, procedure-related complications such as pancreatitis or pseudocyst formation occur in 0% to 18.2% of cases.31112131415
In conclusion, ERCP using BAE is a feasible and useful intervention in patients with Roux-en-Y anastomosis. However, to improve the success rate of this method, technical advances are needed, including the development of long accessories that are compatible with the enteroscope.
 XML Download
XML Download