

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hilar cholangiocarcinoma (HCCA) is the most common type of bile duct cancer, accounting for 46% to 97% of all bile duct cancers.1,2 Surgical resection is only possible in 20% to 30% of patients with HCCA. Therefore, palliative bile drainage intervention is required for patients with unresectable HCCA. The three established methods used for palliation of HCCA are endoscopic drainage, percutaneous drainage, and surgical bypass. However, there is a lack of well-designed comparative or randomized studies regarding the optimal method. Although the Asia-Pacific Working Group on Hepatobiliary Cancer recently made several recommendations,1 establishing a consensus regarding palliation of HCCA remains a challenge. In this review, we describe several points of concern for biliary drainage in HCCA based on evidence and personal experience, and discuss the palliative drainage methods for advanced HCCA, mostly for patients with higher than Bismuth type III HCCA.
HOW MUCH OF THE LIVER SHOULD BE DRAINED IN A PATIENT WITH HCCA AND IS MULTISECTORIAL DRAINAGE NECESSARY?
The right, left, and caudate lobes of the liver occupy approximately 55% to 60%, 30% to 35%, and 10% of the liver volume, respectively.3 One study showed that only 25% of the liver volume can be drained for palliation of jaundice not accompanied by cholangitis.4 However, another study reported a greater decrease in bilirubin level, lower incidence of early cholangitis, and longer patient survival when >50% of the liver volume was drained, compared to draining <50%.5 The Asia-Pacific Working Group on Hepatobiliary Cancer also recommends draining >50% of the liver volume.1
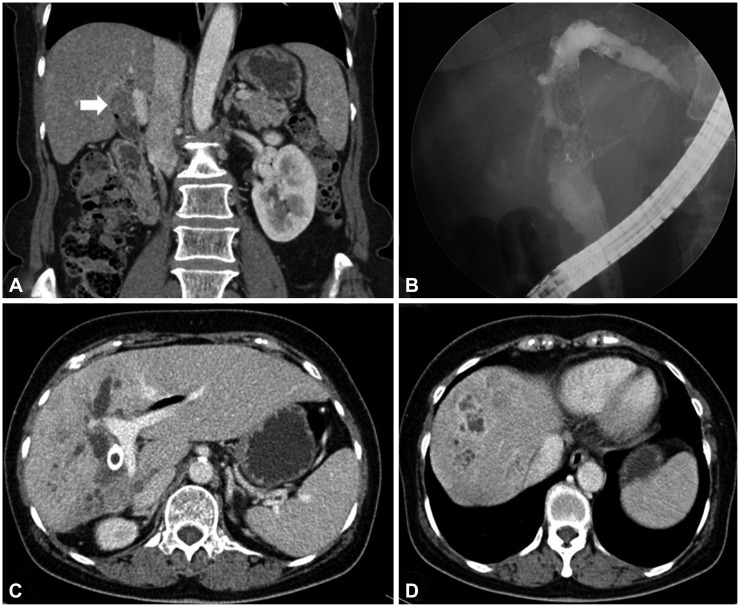
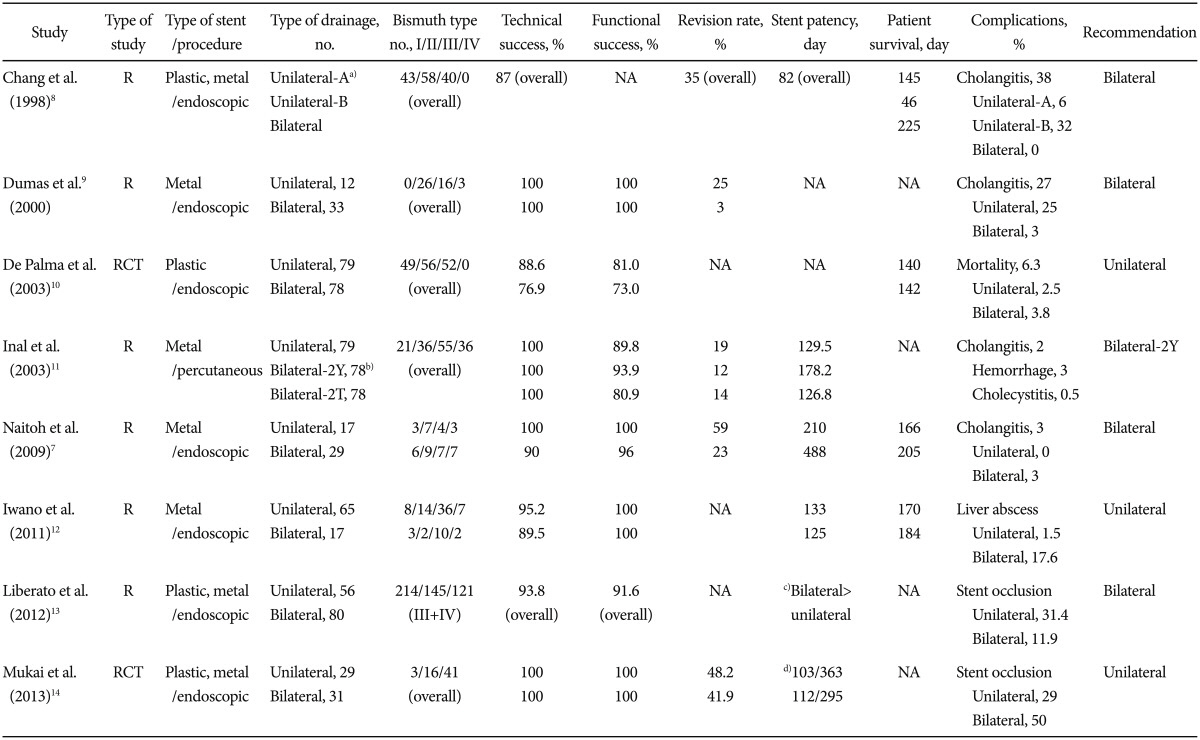
A close relationship between drained liver volume and the number of stents has been identified. Increased bilateral, rather than unilateral, stenting is required to increase drained liver volume. A single stent alone can drain both lobes in a patient with Bismuth type I HCCA, but draining patients with Bismuth types II to IV requires multiple stents. Unilateral stenting has a high technical success rate for stent placement and low early complication rates.6 However, there is a limitation on sufficient drainage >50% of liver volume for patients with Bismuth type II and higher. Additionally, if an infected bile duct cannot be drained, the risk of cholangitis and liver abscess may increase (Fig. 1). In contrast, bilateral stenting preserves functional liver volume, lowers the risk of cholangitis, and reduces complications by draining the infected duct when there is inflammation in a bilateral infected duct, extending patient survival (Table 1).7,8,9,10,11,12,13,14
Injecting contrast dye into undrained ducts can increase the incidence of postprocedural cholangitis and lower the survival rate.15 Preoperative staging and procedural planning with noninvasive imaging, such as magnetic resonance cholangiography (MRCP) or computed tomography (CT), are important in lowering the risk of cholangitis by unsuccessful endoscopy.16,17,18,19,20 These imaging techniques prevent inadvertent injection of contrast into atrophied or multiple unintended hepatic segments. Furthermore, selectively targeted and planned drainage lowers the risk of cholangitis or septicemia by identifying the inflamed bile duct. Therefore, excluding an atrophied segment of lobe or segment and effectively draining the dominant liver lobe lowers the risk of cholangitis and extends patient survival. These benefits arising from bilateral drainage with metallic stents are technically achievable with appropriate endoscopic expertise, development of metal stents, and higher technical and functional success rates, even in patients with Bismuth types III or IV.21,22,23,24,25,26,27,28,29 Thus, the number of biliary stents inserted for palliation and drained liver segments in patients with HCCA must be determined based on the extent of malignant biliary strictures observed on pre-procedural imaging and the degree of biliary tract contamination during biliary drainage.
SELF-EXPANDING METAL STENTS ARE BETTER THAN PLASTIC STENTS FOR ADVANCED HCCA
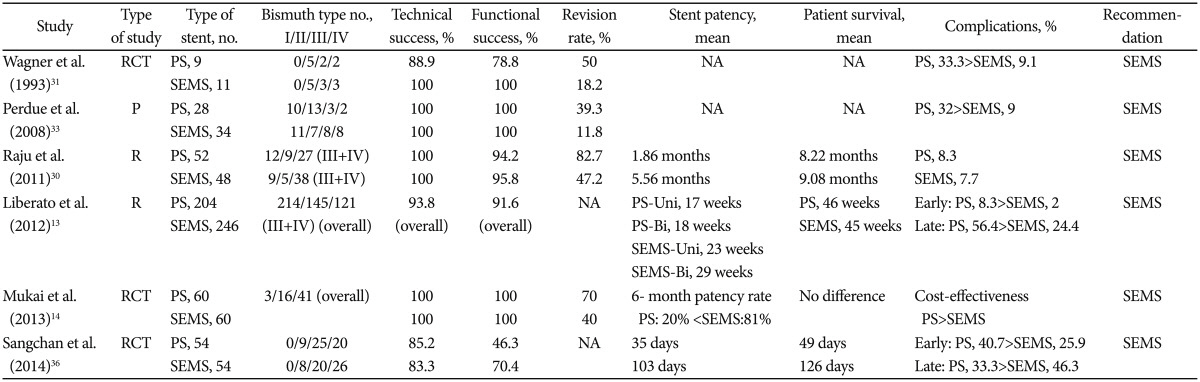
The types of stents used for palliation in HCCA include plastic stents (PSs) and uncovered self-expanding metal stents (SEMSs). PS are less expensive and their insertion and removal are technically easier compared to SEMS. However, because the diameter of PS is smaller than that of SEMS (10 to 12 Fr vs. 8 to 10 mm, respectively), PS occlude more rapidly than SEMS and has a shorter median patency time (1.4 to 3 months vs. 6 to 10 months, respectively).30 Moreover, insertion of more than two 10-Fr diameter PS is difficult and can increase migration rates.31,32 In contrast, SEMS used for HCCA are uncovered, allowing drainage of side branches. SEMS have superior success rates, minimal adverse effects, fewer requirements for re-intervention, and higher patient survival compared to PS.33 Despite the high initial cost, SEMS have superior cost-effectiveness due to the greater success rate, shorter hospital stay, fewer blockages, fewer re-interventions, and lower antibiotic needs compared to PS, when expected patient survival is >4 to 6 months (Table 2).34,35,36 The Asia-Pacific Consensus also recommends biliary pal-liation with SEMS for patients with predicted survival >3 months and Bismuth types II to IV HCCA.1 However, if biliary drainage is performed when a treatment plan for HCCA has not been definitely determined, PS can be temporarily inserted, as PS are removable while SEMS are not.37
INSERTION OF MULTIPLE SEMS: SIDE-BY-SIDE OR STENT-IN-STENT
There are two methods of insertion of multiple SEMS for HCCA. The "side-by-side" method requires insertion of the first stent in one of the hepatic ducts and insertion of the second stent into the contralateral hepatic duct parallel to the first stent.9,38,39,40 The "stent-in-stent" method requires insertion of the second stent in the contralateral hepatic duct through mesh of the first stent.23,41,42,43,44,45,46 Insertion of a stent in bilateral side-by-side stent placement is easier when guidewires are inserted into the right and left hepatic ducts. Endoscopic revision of the stents is also easier on stent occlusion.38 However, disadvantages include the potential for interference when inserting the delivery system for the second stent due to resistance from the already inserted first stent and difficulties in aligning the distal ends of the two stents. A simultaneous side-by-side deployment method using a thin 6-Fr delivery system was developed to overcome these issues and has shown a high success rate.39 However, side-by-side deployment can occlude a portal vein and increase the rate of cholangitis because of excessive expansion of the bile duct by the parallel stents. The excessive expansion force of two deployed SEMS, particularly large-diameter SEMS with a closed metal mesh design, can cause severe pain and vascular injury, possibly leading to massive bleeding.
Effective drainage can be difficult using the side-by-side method in a non-dilated common bile duct and an insufficiently deployed stent can block bile duct flow. Bilateral stent-in-stent deployment is less likely to cause these complications because the stents overlap within the common bile duct. However, it is technically difficult to insert a guidewire for the second stent into the contralateral bile duct through the mesh of the first stent. Moreover, endoscopic revision for an occluded stent is difficult compared to the side-by-side method. Large open-celled wire mesh stents were designed to resolve these issues, using a guidewire to facilitate insertion of the second stent and improve the success rate. This mesh design enables an easy re-intervention. However, the expanding radial force is reduced because of the large cell and susceptibility to tumor in-growth increases.
The success rates for the side-by-side and stent-in-stent methods are 73.3% to 100% and 80% to 100%, respectively.9,38,39,40,41,42,43,44,45,46,47 Although the incidence of complications is higher for the side-by-side method than the stent-in-stent method, stent patency rates are superior.48 No well-designed large-scale comparative studies with long-term follow-up have been performed; therefore, no definite consensus has been reached. Nevertheless, it is expected that attempts to improve the success rate with modifying stents and technical developments of the stent-in-stent method will result in its more frequent use.
ENDOSCOPIC INSERTION OF A SEMS MAY NOT ALWAYS BE THE INITIAL APPROACH
Endoscopic palliation is a less invasive, one-step procedure compared to percutaneous intervention and commonly used as initial treatment for palliation of HCCA. However, it is essential to accurately define the extent of biliary ductal involvement before deciding between endoscopic or percutaneous methods as the initial palliative method of HCCA. A MRCP or CT examination may be helpful in determining the initial method depending on the Bismuth classification of HCCA. Endoscopic treatment is generally the preferred approach for percutaneous drainage for Bismuth types I and II. However, only the technical aspects and success rates have concerned patients with advanced HCCA (Bismuth type III and IV), while technical difficulties and associated complications have been neglected. Complications, such as bleeding and perforation from an endoscopic retrograde cholangiopancreatography for endoscopic drainage and the high incidence of postprocedural cholangitis, are a problem. A multicenter retrospective study found that percutaneous procedures have significantly higher success rates and a lower risk of cholangitis than endoscopic drainage in patients with advanced HCCA.49 Therefore, the Asian-Pacific Consensus recommends that endoscopic palliation be considered as an initial treatment for less-advanced Bismuth types (I and II) and that percutaneous palliation be considered for advanced Bismuth types (III and IV).1 However, endoscopy is the initial approach, even in patients with advanced Bismuth types in actual clinical practices at many institutes, including ours. Nevertheless, we prefer to convert endoscopy to a percutaneous approach when any difficulties are encountered during the procedure. This policy is better than a "never give up policy" for patient safety and preventing procedure-related adverse events. Unlike previous studies describing only short-term outcomes, large-scale randomized studies are needed to investigate long-term outcomes regarding the duration of efficient drainage and the possibility of effective re-intervention when a stent becomes obstructed.
WHEN SHOULD WE CALL AN INTERVENTIONAL RADIOLOGIST?
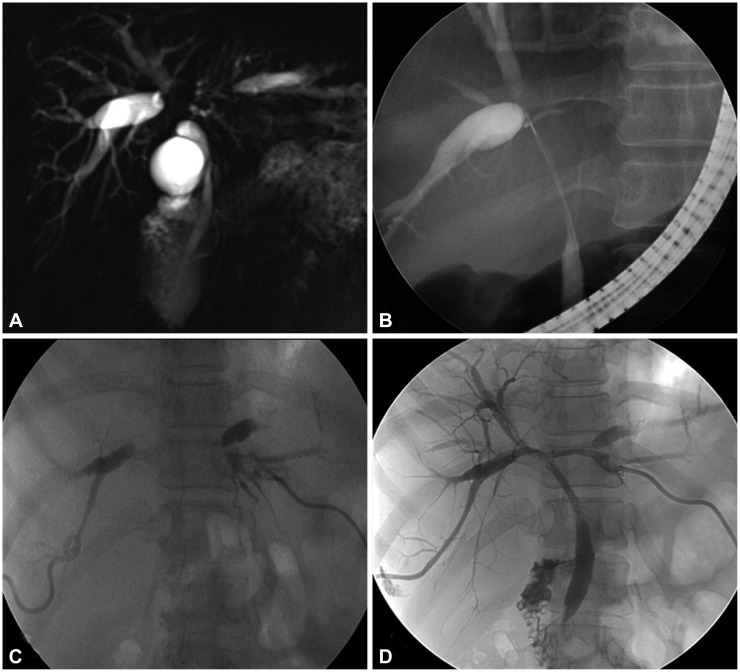
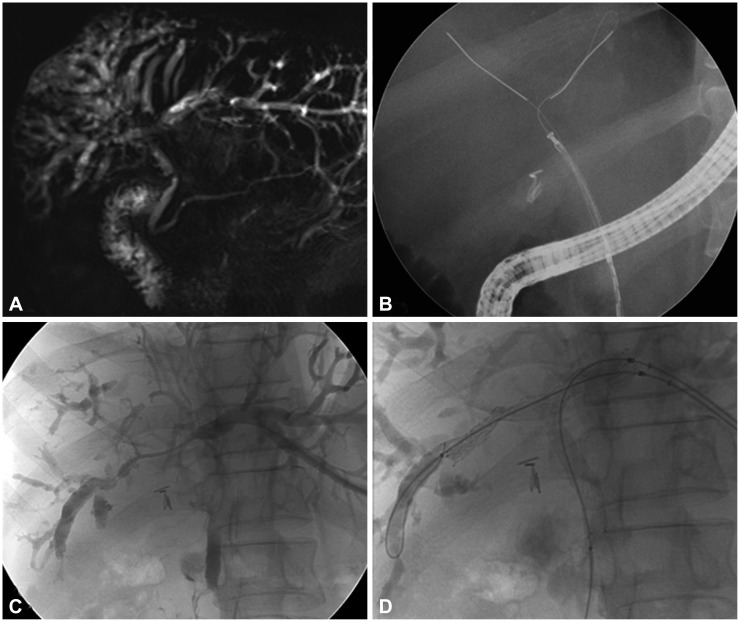
Drainage is necessary because the complication rate, including postprocedural cholangitis, increases when contrast dye is injected into undrained bile ducts.34 Therefore, percutaneous drainage must be performed immediately after unsuccessful endoscopic drainage to prevent postprocedural cholangitis and improve the palliative success rate.49 The success rate of palliation is higher in a percutaneous approach in patients with advanced HCCA (Bismuth types III and IV) compared to an endoscopic approach. This is due to: (1) puncture at a precisely selected bile duct; (2) easier guidewire and catheter approach; and (3) a greater variety of designs for drainage (T- or X-shaped).50 Our comparative study of patients who underwent successful initial endoscopic SEMS stenting (group I) and patients who underwent unsuccessful initial endoscopic SEMS stenting but successful subsequent percutaneous SEMS stenting (group II) showed that the success rate of endoscopic stenting for patients with advanced HCCA (Bismuth types III and IV) was lower than that for percutaneous stenting (72.4% vs. 100%, respectively; p<0.05, unpublished data). Importantly, sequential stenting by the percutaneous method was possible for all patients who failed in the endoscopic retrograde method through endoscopic retrograde cholangiopancreatography. Although strictures in these patients were tight and had a long segment preventing the guidewire from being passed in the endoscopic method, the percutaneous anterograde method may overcome these limitations (Figs. 2, 3). These results are similar to previous studies.49 Therefore, the percutaneous approach should be considered as initial palliation for some patients with advanced and difficult Bismuth types III and IV HCCA. Moreover, sequential percutaneous intervention is important for successful palliation when an endoscopic approach fails.
CONCLUSIONS
The top priority for palliation of unresectable HCCA is to determine a drainage plan prior to the procedure using non-invasive imaging, such as MRCP or CT. Moreover, it is important to consider several factors, such as the patient's bile duct, hepatic anatomical information, the patient's condition, existing medical sources, and the endoscopist's expertise, when selecting the appropriate bile duct for drainage, type and number of stents, and drainage method for the most effective pallia-tion. All attempts must be made to drain the infected bile duct, and a percutaneous method should be considered first for patients with advanced HCCA (Bismuth types III and IV). In particular, if the intention to treat initially fails using endoscopy, it is essential to switch immediately to a percutaneous method.
 XML Download
XML Download