

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Until recently, gastric cancer comprised the second most common type of cancer worldwide. In 2012, gastric cancer fell to fifth place, behind lung, breast, colorectum, and prostate cancers.1 Nevertheless, gastric cancer remains the third most common cause of cancer death.1 Asian countries, including China, Japan, and Korea, in particular, report some of the highest incidences of gastric cancer in the world.2 While its incidence has declined in Korea in recent decades, gastric cancer was still the second most common cancer in the country in 2010 (crude incidence rate: 60.3 per 100,000; age-standardized incidence rate: 41.8 per 100,000).3
In countries with high prevalence rates of gastric cancer, like China, Japan, and Korea, gastric cancer screening is common. Since 1960, as a result of mass gastric cancer screening implementation using photofluorography (via indirect upper gastrointestinal series [UGIS]), which facilitates early detection, Japan has achieved improvements in survival and cure rates.4,5,6 In recent years, endoscopy has been increasingly utilized in opportunistic screening for gastric cancer.7 In Korea, the nationwide gastric cancer screening program has provided endoscopy and UGIS as initial screening methods.8 However, apart from the countries where gastric cancer is highly prevalent, many countries generally lack national guidelines or recommendations for gastric cancer screening. Additionally, data in support of the effectiveness of gastric cancer screening are lacking.
Thus, the aim of this review was to examine current evidence on gastric cancer screening and to determine the most cost-effective screening strategies. Herein, we reviewed radiographic and endoscopic tests as screening methods for gastric cancer, as these two methods are most commonly provided by population-based organized screening programs.
CURRENT POPULATION-BASED GASTRIC CANCER SCREENING PROGRAMS
The incidence and mortality of gastric cancer differ significantly by region, population, and race distribution. Additionally, healthcare systems, health resources, and social and economic conditions may greatly affect gastric cancer prevention and screening strategies. At present, the East Asia region, particularly Japan, Korea, and other countries with high incidence rates of gastric cancer, have achieved tangible results from their screening programs, as well as from preventive interventions. However, no nationwide screening of gastric cancer has been reported in the United States, Europe, or other areas with low incidence rates of gastric cancer.
Japan
Around 1960, gastric cancer screening via photofluorography began to be offered in the Miyagi prefecture and has since been adopted nationwide.9 In 1983, under the Health Service Law for the Aged, annual gastric cancer screening via photofluorography was introduced for all residents aged 40 years and older. The screening rate for gastric cancer was 11.8% in 2007, following a trend of declining participation in screening programs since the early 1990s.10 In 2008, a Japanese research group for cancer screening recommended guidelines for gastric cancer screening.9 To do so, they evaluated four gastric cancer screening methods: photofluorography, endoscopy, serum pepsinogen testing, and Helicobacter pylori antibody testing. On the basis of a benefit/harm balance, the research group recommended gastric cancer screening using photofluorography for both population-based and opportunistic screening.9 The other methods were not recommended for population-based screening because of insufficient evidence.9 Notwithstanding, endoscopy has recently replaced photofluorography as the initial mass screening method in several Japanese cities.11
Korea
In Korea, the Korean Gastric Cancer Association and National Cancer Center established national guidelines for gastric cancer screening in 2001. These guidelines recommend biennial gastric cancer screening for men and women aged 40 years or older via either UGIS or endoscopy.12 Based on these guidelines, a nationwide gastric cancer screening program was started in 2002 as part of the National Cancer Screening Program (NCSP). The NCSP now provides support for biennial gastric cancer screening via either UGIS or endoscopy for Medical Aid Program recipients and National Health Insurance beneficiaries aged 40 or older.13 The participation rate for gastric cancer screening provided by the NCSP increased from 12.7% in 2002 to 43.9% in 2012.14,15 In addition to the NCSP, opportunistic gastric cancer screening is also widely available in Korea. According to the Korean National Cancer Screening Survey, the participation rate for opportunistic and organized gastric cancer screening has increased significantly, from 39.2% in 2004 to 70.9% in 2012.16
Other countries in Asia
In China, although gastric cancer is the second most common cancer, no nationwide screening program has been established. Therefore, early detection of gastric cancer relies on opportunistic screening alone, although endoscopy is widely available in major cities. Notwithstanding, UGIS and serum pepsinogen testing are not commonly practiced in China for reasons of cost and availability.7
Singapore also lacks a nationwide gastric cancer screening program for the population.7 As the risk of developing gastric cancer in Singapore is deemed intermediate, screening is more effectively targeted at high-risk groups than at the population level. A cost-benefit analysis of gastric cancer screening conducted in Singapore showed that screening by endoscopy was most cost-effective in moderate- to high-risk populations.17
In Taiwan, gastric cancer screening is limited to the high-risk population. Two prevention campaigns have been implemented in Matzu Island where the prevalence and incidence of gastric cancer were exceptionally high.18,19 From 1995 to 2004, subjects with low serum concentrations on the serum pepsinogen test (<30 ng/mL) received endoscopy.18 From 2004 to 2005, those with H. pylori infection underwent endoscopy and H. pylori eradication,19 and this population-based program showed that H. pylori eradication significantly reduced the incidence of atrophic gastritis and gastric cancer.20
EVIDENCE ON GASTRIC CANCER SCREENING
The efficacy of cancer screening is best assessed with randomized controlled trials to determine mortality reductions in screened versus unscreened subjects. Although randomized controlled trials represent the most reliable method for evaluating the impact of screening on cancer risk, such intervention studies are not feasible in most countries because gastric screening is already widely conducted. Furthermore, obtaining accurate estimates of mortality reductions requires long-term follow-up of large populations.
Radiographic tests (photofluorography, UGIS, or barium-meal studies)
No randomized controlled trial addressing the use of radiographic tests in gastric cancer screening has been published. Meanwhile, four case-control studies and four cohort studies have been conducted to evaluate the effect of gastric cancer screening by photofluorography on mortality (Table 1); one case-control study was conducted in Venezuela,21 while the others were conducted in Japan.4,22,23 Most of the case-control studies conducted in Japan demonstrated a 40% to 60% reduction in gastric cancer mortality with photofluorography screening.4,23,24 Nonetheless, the study conducted in Venezuela reported no detectable reduction in gastric cancer mortality. Fukao et al.,4 Oshima et al.,22 and Abe et al.23 reported that the summary odds ratios of three case-control studies for ever-screened versus never-screened subjects were 0.39 (95% confidence interval [CI], 0.29 to 0.52) for men and 0.50 (95% CI, 0.34 to 0.72) for women in reducing gastric cancer mortality.24 They discerned that the Japanese screening program with photofluorography is effective in reducing gastric cancer mortality.
Regarding the four cohort studies, one study lacked statistical power and did not show a significant difference in the relative risk (RR) of mortality.25 The cohort study conducted by Mizoue et al.5 revealed significantly reduced mortality in men (RR, 0.54; 95% CI, 0.41 to 0.70), while the reduction in mortality was not significant in women (RR, 0.74; 95% CI, 0.51 to 1.07). Another cohort study with a 13-year follow-up in Japan reported a 40% reduction in gastric cancer mortality in screened versus unscreened subjects (RR, 0.60; 95% CI, 0.43 to 0.83).26 The most recent study, conducted by Miyamoto et al.,27 also reported a significant mortality reduction in both men and women who had undergone screening versus those who had not (RR, 0.52; 95% CI, 0.36 to 0.75 in men; RR, 0.51; 95% CI, 0.27 to 0.96 in women).
Endoscopy
Only a few studies have evaluated the effectiveness of endoscopic screening in terms of mortality reduction (Table 2). One community-based case-control study was conducted to evaluate the reduction in gastric cancer mortality by endoscopic screening.28 In this study, compared to patients who had never undergone screening for gastric cancer, the odds ratios were 0.695 (95% CI, 0.489 to 0.986) for patients who underwent endoscopic screening and 0.865 (95% CI, 0.631 to 1.185) for those who underwent radiographic screening.
Regarding cohort studies, one study was conducted in an area with a high incidence of gastric cancer in Linqu County, China.29 From 1989 to 1999, endoscopic screening was conducted for 4,394 residents. Both the incidence and mortality rates of gastric cancer were monitored until 2000. Over this period, 85 cases of gastric cancers were detected, 29 of which were early cancers. However, compared with the overall mortality for Linqu County, the standard morality ratio was 1.01 (95% CI, 0.72 to 1.37). Another cohort study conducted in Japan by Hosokawa et al.30 reported that the RR for gastric cancer death in the examined group was 0.347 (95% CI, 0.140 to 0.860) when compared with the nonexamined group. The RRs in men and women were 0.217 (95% CI, 0.068 to 0.699) and 0.684 (95% CI, 0.160 to 2.929), respectively. In conclusion, they recommended the application of endoscopy in population-based screening programs for gastric cancer in regions or countries where gastric cancer mortality is high.
TEST ACCURACY
Usually, the accuracy of a screening test is indicated by its sensitivity and specificity. A good screening test must have high sensitivity and high specificity. The most common method used to calculate sensitivity and specificity involves the follow-up of persons who have undergone screening to ascertain the number of cancer cases occurring among them via record linkage to a population-based cancer registry. Table 3 summarizes the reported sensitivities and specificities of radiographic and endoscopic tests as screening methods.
The sensitivity of photofluorography reported from the Japanese studies ranged from 56.8% to 88.5%, whereas specificity ranged from 81.3% to 92.0%.31,32,33,34,35,36 Two studies related to the use of endoscopy as a diagnostic test have reported on the accuracy of endoscopy.37,38 In the first study, the sensitivity of endoscopy was found to be 77.8%, based on a 3-year follow-up using the cancer registry system of the Fukui prefecture.37 The other study based on a follow-up survey of individual participants recorded an 84.0% sensitivity for endoscopy.38
Two recent studies have compared the accuracies of radiographic tests and endoscopy.39,40 One study conducted in Korea utilized data obtained from a population-based national cancer screening database. In that study, the sensitivities of UGIS and endoscopy screening to detect gastric cancer were 36.7% and 69.0%, with specificities of 96.1% and 96.0%, respectively. The other study conducted in Japan reported sensitivities of prevalence screening calculated by the incidence method of 89% for endoscopic screening and 83% for radiographic screening; however, the difference was not significant. The specificities of endoscopy and radiographic screening were 85% and 86%, respectively. The differences in the sensitivities and specificities between Korea and Japan might be affected by the differences in their respective screening intervals: every 2 years in Korea and every year in Japan. Also, the quality of cancer registry data in the Japanese study was not good, as some of the interval cancers were lost because of insufficient follow-up, and the sensitivity might have been overestimated. Nevertheless, both studies showed that the sensitivity of endoscopic screening for gastric cancer was higher than that of radiographic screening and suggested there should be greater use of endoscopy in gastric cancer screening.
COST-EFFECTIVENSS AND PREFERENCE
In the United States, where gastric cancer incidence rates are low, one study comparing endoscopy versus no screening concluded that one-time screening for the general population at the age of 50 would cost US $115,664 per quality-adjusted life year (QALY).41 Another study in the United States concluded that endoscopy screening of less advanced lesions was not cost-effective, except possibly for immigrants from high-risk Asian countries.42
In many Asian countries experiencing high gastric cancer burden, cost-effectiveness analyses of gastric cancer screening are ongoing. In Singapore, where the risk of gastric cancer is low to intermediate, annual endoscopy was deemed the optimal strategy, with an incremental cost-effectiveness ratio (ICER) of US $44,098 per QALY compared to no screening, while biennial endoscopy was estimated as the most cost-effective strategy with an ICER of US $25,949 per QALY.43 The ICERs per QALY in the Singaporean study were lower than those in the United States because of differences in gastric cancer prevalence, healthcare resources, screening strategy costs, and other healthcare-related factors. A study conducted in Taiwan reported that annual screening using endoscopy for high-risk populations whose pepsinogen-I levels were <30 ng/mL at the age of 50 years versus no screening resulted in an ICER of US $29,741 per life year gained.44 In a Japanese study, endoscopy was deemed the best method for detecting early gastric cancer and the cheapest strategy with regard to the cost of identifying one case of gastric cancer.11
The Korean government provides gastric cancer screening as a part of the NCSP and requires many studies to report on the cost-effectiveness thereof. Lee at al.45 reported that endoscopy was more cost-effective than UGIS until the cost per cancer case detected becomes 3.7-fold more expensive than UGIS. Another study by Chang et al.46 using a time-dependent Markov model to compare 13 different screening alternatives reported annual endoscopy from ages 50 to 80 years was the most cost-effective strategy in men, and biennial endoscopy from ages 50 to 80 years was the most cost-effective in women. Cho et al.47 reported that endoscopy ICERs (119,099,000 to 178,700,000 Korean won/survival) were lower than upper gastrointestinal X-ray ICERs (260,201,000 to 371,011,000 Korean won/survival). In Korea, three studies comparing endoscopy versus no screening agreed on endoscopy as the more cost-effective strategy.
In financial terms, the test is not as cost-effective if the cost is too high. The cost of endoscopy is reportedly 3- to 4-fold more expensive than that of radiography testing (photofluorography) in Japan.11,48 However, in Korea, the cost of endoscopy is about the same as that of radiographic testing (UGIS) (unit costs for endoscopy and UGIS were US $34.89 and US $32.67, respectively, in 2008).45
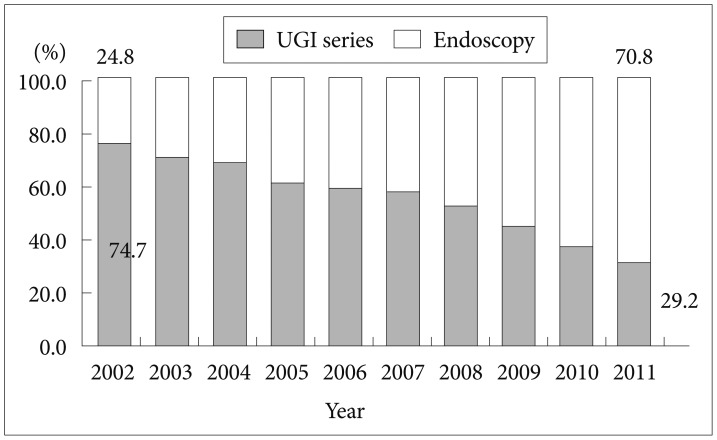
For a successful screening program, a high level of participation is required, which likely depends on individual attitudes and preferences about the screening method used. In Korea, endoscopy is the preferred method for gastric cancer screening. According to a Korean National Cancer Screening Survey in 2006, 67% of individuals chose endoscopy as their preferred gastric cancer screening method, while 33% chose UGIS as their preferred method.49 Furthermore, the proportion of people choosing endoscopy screening provided by the NCSP has continued to increase annually, from 24.8% in 2002 to 70.8% in 2011 (Fig. 1).50
CONCLUSIONS
Endoscopy is widely conducted in clinical settings as a part of routine health check-ups. Some authors have reported higher detection rates of early-stage gastric cancer with endoscopy compared to radiographic tests and have thus concluded that endoscopy is a more sensitive screening method.11,39,40,51 Despite the diagnostic advantages of endoscopy, data on the impact of endoscopy screening programs on gastric cancer mortality are limited.
Notwithstanding, the results of recent studies suggest that application of endoscopy in gastric cancer screening programs is more cost-effective than screening by radiographic tests in average-risk populations. Also, the general population is more likely to prefer gastric cancer screening by endoscopy. Nonetheless, further study of the impact of endoscopy on gastric cancer mortality is needed, and future evaluations of screening methods should take into account cost and any associated reduction in gastric cancer mortality.



 XML Download
XML Download