

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary fallopian tube carcinoma (PFTC) is a rare cancer constituting about 0.14% to 1.8% of all gynecological cancers.1 The incidence of PFTC likely underestimates the frequency of the disease because it is often difficult to distinguish whether a tumor is of tubal or ovarian origin, particularly among women with metastatic disease.
Routine imaging for suspected PFTC includes vaginal ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) of the abdomen.2 Elastography is an imaging modality for the evaluation of tissue stiffness, and has been used to analyze superficial organs, including the breast and the prostate.3,4 Measurement of tissue elasticity has been reported to be useful for the diagnosis and differentiation of tumors, which are stiffer than normal tissues.5 Endoscopic ultrasound (EUS) elastography is a promising imaging technique with high accuracy for the differential diagnosis of solid pancreatic tumors6 and that has been studied for the diagnosis of other tumors.7 Here, we report the case of a 66-year-old female patient with PFTC that was diagnosed preoperatively with the aid of EUS elastography and fine needle biopsy (FNB).
Go to : 
CASE REPORT
A 66-year-old multiparous female patient was referred to our hospital for the evaluation of recurrent vaginal bleeding and dull lower abdominal pain for 2 months. She had recently undergone vaginal sonography at a private gynecologic clinic, where a malignant adnexal mass was suspected. On admission, the results of a physical examination were unremarkable and her vital signs were normal. Laboratory testing showed a CA-125 level of >1,000 U/mL (reference value, 0 to 35). A Pap smear test did not reveal any evidence of malignancy, except for atrophy and inflammation. Both abdominopelvic CT and pelvic dynamic MRI revealed an 8×5×5 cm heterogeneous irregular enhancing mass, at the cul-de-sac extending to both adnexa, that had directly invaded the rectal wall (Fig. 1). The patient underwent a colonoscopy to detect rectal invasion by the mass and as a preoperative baseline study. Colonoscopy revealed a bulging lesion visible within the rectal lumen, covered by a relatively normal-appearing mucosa although focal erythema was noted on the overlying mucosa.
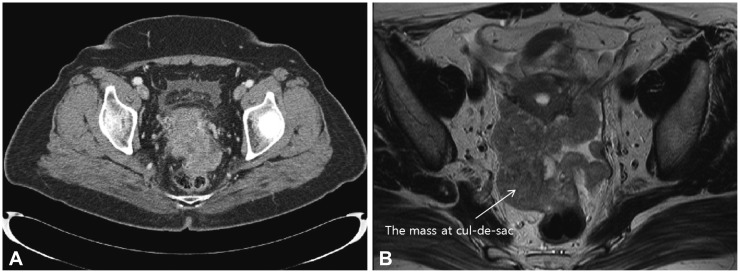 | Fig. 1Computed tomography (CT) and magnetic resonance imaging (MRI) of the adnexal mass. (A) An about 8-cm, heterogeneous enhancing mass with irregular shape, involving from the uterine cervix to the uterine fundus, was detected by using CT. (B) The mass at cul-de-sac (white arrow) has directly invaded to the rectum on MRI.
|
EUS was performed to evaluate the subepithelial tumor of the rectum, by using an electronic radial-type echoendoscope (EG-3670 URK; Pentax, Tokyo, Japan) and EUB-7500 ultrasound (Hitachi Co., Tokyo, Japan) with the real-time tissue elastography module. EUS revealed a sausage-shaped hypoechoic mass, 8 cm in size, with irregular margins and heterogeneous internal echoes extending to both adnexa (Fig. 2A). The solid echogenic adnexal mass had nearly obliterated the lumen of both fallopian tubes and had invaded the fundus of the uterus. The lesion primarily invaded the right side of the uterine body; however, it was difficult to delineate the borderline between the lesion and the uterus (Fig. 2B). Dual imaging with the conventional gray-scale B-mode EUS image (right) and elastographic image (left) demonstrated that the mass had a blue color pattern, representing hard stiffness, and heterogeneous green/red coloration outside the tumor, representing intermediate stiffness (Fig. 2C).
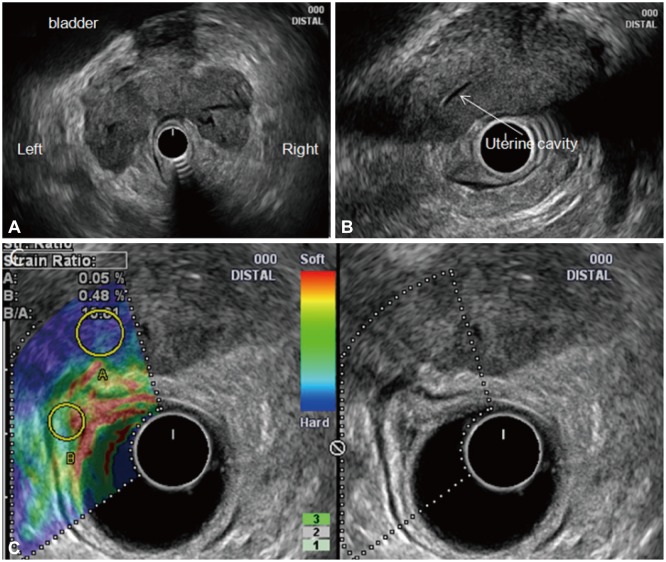 | Fig. 2Endoscopic ultrasound elastography of the adnexal mass. (A) A sausage-shaped hypoechoic mass, 8 cm in size, with irregular margins and heterogeneous internal echoes extending to both adnexa and that had obliterated the lumen of both fallopian tubes was detected. (B) The mass had invaded the right side of the uterine body, making it difficult to delineate the borderline between the lesion and the uterus. (C) Elastographic image of the left side of the dual image showing the blue color pattern (representing hard stiffness) of the mass and heterogeneous green/red coloration (representing intermediate stiffness) outside the tumor.
|
Tissue stiffness was quantitatively assessed by calculating the strain ratio. Two different areas (A and B) from the region of interest were selected for quantitative elastographic analysis. Area A is representative of the mass and area B refers to a reference area outside the tumor. The B/A strain ratio is considered to be a measure of tissue elasticity; in our case, the B/A ratio of the adnexal mass was 15.61. A strain ratio value has not been reported for a malignant adnexal mass; however, on the basis of strain ratio data reported for pancreatic cancer,8 these findings suggested the presence of a malignant adnexal mass. An EUS-guided FNB with a ProCore needle (Cook Endoscopy, Limerick, Ireland) was subsequently performed, which identified papillary tumor cells with hyperchromatic nuclei and frequent mitosis, suggestive of a primary or metastatic papillary adenocarcinoma of the pelvic cavity (Fig. 3A). Given the patient's medical history, increased level of CA-125, and the results of CT/MRI and EUS elastography with tissue biopsy, the adnexal mass was diagnosed as PFTC with uterine involvement. On the basis of this finding, the patient underwent a total abdominal hysterectomy with bilateral salphingo-oophorectomy, omentectomy, and pelvic regional lymph node dissection.
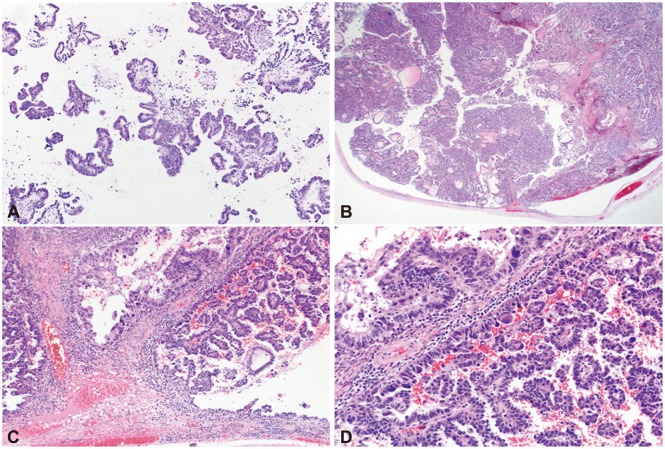 | Fig. 3Histopathologic analyses of needle biopsy and operative tissue specimens. (A) The ProCore needle biopsy specimen revealed papillary growing tumor cells with hyperchromatic nuclei and frequent mitoses, suggestive of primary or metastatic papillary adenocarcinoma of the pelvic cavity (H&E stain, ×100). (B) The operative specimen revealed a tumor occupying the lumen of the right residual fallopian tube that had extended to the pelvic cavity (H&E stain, ×12.5). (C) Operative specimen showing the tumor arising from the luminal epithelium with a papillary growth pattern (H&E stain, ×100). (D) Operative specimen showing that the tumor consisted of a fibrovascular core lined by a single layer of tumor cells with occasional pleomorphic cells and frequent atypical mitosis (H&E stain, ×200). These findings are similar to those of the endoscopic ultrasound-guided biopsy.
|
Gross examination of the tissue specimens showed extensive adhesion of the tumor mass with both residual fallopian tubes. However, both ovaries and the endometrium were unremarkable. Microscopically, the tumor mass arose from the luminal epithelium of the right fallopian tube (Fig. 3B, C) with a fibrovascular core lined by a single layer of tumor cells displaying a moderate amount of cytoplasm, hyperchromatic nuclei, and occasional prominent nucleoli. Pleomorphic cells and atypical mitosis were frequently noted. These findings are similar to those produced with EUS-guided biopsy (Fig. 3D) and confirmed the diagnosis of a serous adenocarcinoma of fallopian tube origin with pelvic extensions. There were no metastatic tumors in the pelvic lymph nodes (0 of 7); however, metastases were found in regional lymph nodes (24 of 32) and the omentum (24 of 25) with positive abdominal cytology. The cancer was staged as IIIC according to the guidelines from the International Federation of Gynecological Oncologists.
Go to :
DISCUSSION
PFTC is diagnosed preoperatively in only 4% of patients, and up to 50% of cases are missed intraoperatively.9 Surgical intervention consists of total abdominal hysterectomy, bilateral salpingo-oophorectomy, and comprehensive surgical staging.10,11,12,13 However, an initial misdiagnosis causes patients to undergo multiple surgeries because correct staging of the cancer is often not performed at the time of the initial operation. In advanced disease, postoperative residual disease >2 cm can have an adverse prognostic impact,10,11,12,13 and aggressive debulking should be attempted in patients with an advanced tumor.
This is the first report about the role of EUS in the diagnosis of PFTC. The sonographic appearance of PFTC can be nonspecific and may mimic other pelvic diseases such as a tubo-ovarian abscess, ovarian tumor, and ectopic pregnancy. The reported ultrasound features include a sausage-shaped mass, cystic spaces with mural nodules, and a multilobular mass with a cog and wheel appearance in the adnexal region.2,14,15,16 The sonographic presentation of the disease in our patient was unusual because of bilateral fallopian tube and myometrial involvement. Bilaterality has been reported in 10% to 20% of cases; however, in one report, the figure was only about 3%.12 In this case, the solid echogenic adnexal mass, which had irregular margins and a heterogeneous pattern and which had obliterated both fallopian tubes and invaded some portion of the uterus, was suspected to be PFTC with uterine involvement.
It is often difficult to determine the benign or malignant nature of an adnexal mass by using sonography. In our case, we used elastography in the differential diagnosis of the malignant adnexal mass. Elastography is the diagnostic modality for tissue hardness. Generally, tissue hardness is thought to correlate with malignant potential as malignant tumors are harder than benign tumors.17 The elastic characteristics of the tissue appear to be fairly uniform throughout benign lesions. By contrast, cancer grows in an unorganized manner so that its elastic properties are rather heterogeneous throughout the tumor. On the basis of this concept, real tissue elastic imaging with EUS or ultrasound has been introduced for clinical use.18 Elastography has recently been used to diagnose malignancies in solid pancreatic, breast, and prostate masses. With this technique, malignant tumors are harder (shown as blue) than benign tumors. In our patient, EUS elastography showed a blue color pattern with a heterogeneous distribution. To our best knowledge, EUS elastography had been used to diagnose gastric metastasis of ovarian cancer in only one case.19 In the case of pancreatic cancer, a strain ratio >6.04 is 100% accurate for classifying malignant tumors, and a strain ratio >15.41 is 100% accurate for assessing the malignancy of a solid pancreatic mass.8 We used the known strain ratio reported for pancreatic cancer to support a diagnosis of a malignant adnexal mass in our patient. Further study of EUS elastography in the assessment of a malignant adnexal mass in additional patients is needed to confirm this result.
FNB with the EUS-guided ProCore biopsy needle has recently been introduced,20 and was used in this report for the pathological diagnosis of an adnexal mass. This needle is made of stainless steel with a nitinol stylet that runs through the cannula of the needle to match the tip bevels. The sheath of the ProCore needle is 5.2 Fr and has a 2-mm reverse bevel side fenestration 3.9 mm from the needle tip to allow the suctioning of tissue into the bevel and to gain core tissue upon withdrawal. The handle materials are Lexan-121, polystyrene, and Dynaflex. In one large multicenter trial, use of the ProCore was deemed a feasible and safe technique for histopathological diagnosis, with high diagnostic accuracy.20
In summary, although gynecologic malignancies are not typically within the scope of endosonographic practice, we used EUS elastography in the evaluation of a patient who presented with a subepithelial tumor of the rectum. Thus, it is essential to be familiar with the sonographic features of fallopian tube carcinoma so that an accurate diagnosis can be made early for the prompt management of these patients.
Go to :
 XML Download
XML Download