

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) is an essential procedure for the diagnosis and treatment of pancreatobiliary diseases; however, it is invasive and may induce complications such as pancreatitis, cholangitis, hemorrhage, and perforation. For successful and safe ERCP procedures, provision of necessary laboratory conditions for pre-operative preparation, preparation of the procedural environment, and risk factor stratification should be performed as the first steps. In light of the recent population aging and increase in chronic diseases in Korea, the cautionary measures to be taken for old persons and patients with cardiovascular disease, to minimize complications in such population groups, along with other precautions concerning endoscopic sedation, will be discussed in this review. Finally, materials and options for guidewires that are commonly available as an accessory for the procedure will be introduced in this literature review.
Go to : 
PRE-ERCP PREPARATION
The procedural environment for a safe and successful ERCP is important for both the operator and the patient. An ERCP room should allow an ample space around the examination table so that basic endoscopic devices, the many assistive devices and accessories, and C-arm fluoroscopy equipment could be operated without difficulty. In this light, an ERCP room should be 50% to 100% greater in area than a conventional endoscopy room, or at least 30 m2 according to a previous report.1 Besides the operating endoscopist, the personnel should include a monitoring staff, two or more assistants (an experienced one and a secondary one), and an anesthesiologist (if needed). Continuous monitoring of the patient is as essential as the mechanical measurements performed for ensuring the safety of patients and minimizing serious complications. However, the current medical environment in Korea may provide limited space and personnel for ERCP alone. Preparing enough space, instruments, and experienced personnel may be the basic step for ensuring safe and effective procedures.
Besides the procedural environment and the operator's experience being important factors for the safety of ERCP and preventing complications, it is also important to predict the patient's likelihood of developing complications as well as to determine whether there is an absolute requirement for ERCP and what other preventive measures are required. If the patient is at a high risk or in a severe condition, diagnostic ERCP can be replaced with magnetic resonance cholangiopancreatography (MRCP) or endoscopic ultrasonography (EUS). Lastly, it is important to identify and deal with the risk factors of complications. Procedural limitations, such as the operator's lack of experience, hospital environment, and difficulty of the procedure, should be identified in advance. It is also necessary to identify patient and procedural risk factors, and prepare a plan accordingly in advance.2,3 For example, the well-known risk factors of post-ERCP pancreatitis are ampullectomy, precut papillotomy, sphincter of Oddi dysfunction (SOD), young age in women, history of post-ERCP pancreatitis, repeated pancreatic duct cannulation, pancreatic contrast injection and acinarization, difficult cannulation, and prolonged cannulation time.1,2,3 The recognition of these predictive factors is helpful for reducing unnecessary procedures and the risk of complications.
Go to :
ERCP IN OLD AGE AND PATIENTS WITH CARDIOPULMONARY DISEASES
The age of 65 years and older is commonly defined as old age. Korea entered the aging society in the early 2000s and is on the brink of entering the super-aged society. Nowadays, old age alone is not a reason for abandoning or delaying most aggressive treatments. Furthermore, diseases that are associated with each other, such as diabetes mellitus, hypertension, hyperlipidemia, heart diseases, and cerebrovascular diseases, increase with age. Aging entails a reduction in the physiological functions of body organs, hepatic metabolism of drugs, and renal excretion of drugs. The gallbladder function also decreases, increasing the formation of gallstone and the prevalence of cholelithiasis. In older persons, acute cholecystitis is more likely to be combined with bile duct stone than in younger persons (10% to 20% vs. 5%), periampullary diverticulum is more frequent, and multiple or large gallstones are often detected. Acute cholecystitis has nonspecific symptoms in many cases, often delaying its detection or causing it to be mistaken for another disease. The prevalence of pancreatobiliary cancer is also increased among older patients. Previous studies reported that the mortality and morbidity of biliary surgery were as high as 9.5% and 62%, respectively, necessitating a more careful consideration before performing biliary surgery in super-aged patients.4,5,6 As older persons are more susceptible to the adverse effects of drugs or drug interactions, for a safe ERCP in older persons and patients with severe cardiovascular diseases, it is necessary to understand their physiological characteristics, analyze their risk factors, and control these risk factors before determining further therapeutic strategy.
ERCP in older persons
Compared with surgeries, ERCP is less associated with serious complications, making it a useful tool for the diagnosis and treatment of pancreatobiliary diseases. However, there are only a limited number of studies on the usefulness and safety of ERCP in patients aged 80 years and older, or in those with severe cardiovascular diseases. As pancreatobiliary diseases are often combined with chronic diseases in older patients, ERCP is relatively more prone to entail complications in such patients than in younger patients. In recent years, diagnostic ERCP is often replaced with MRCP, which has been proved as effective and safe in many studies.7,8,9 However, MRCP or EUS cannot replace therapeutic ERCP. In practice, the overall complication rates of ERCP in patients aged 80 years and older are 5% to 8.7%, which is not as high as might be expected.10 Clarke et al.8 reported about a 5% incidence of pancreatitis after ERCP in patients aged 85 years and older. Sugiyama and Atomi11 reported that there was no difference in the post-ERCP frequency of pancreatitis depending on age. Lukens et al.10 reported that the incidence of pancreatitis was decreased in older patients, further fueling the controversy over the incidence of pancreatitis after ERCP in super-aged patients. In domestic studies, Kim et al.9 found no statistical difference but rather a reducing pattern of complications among older patients. Such results may be explained by the histological changes of the pancreas, such as the change of pancreatic ductal epithelium from normal to squamous epithelial cells and the fibrotic change of the pancreatic parenchyma, and the poor functioning of the pancreatic enzymes with aging.12 These changes may be considered as protective factors against post-ERCP pancreatitis in older patients. Therefore, it is unnecessary to avoid or delay ERCP because of old age for fear of serious complications such as pancreatitis.
Older patients with cardiovascular diseases
ERCP may induce asymptomatic myocardial damage or myocardial infarction in older patients with cardiovascular disease, which has been confirmed by the increase in cTnI, a specific marker for myocardiac cell injury.13 In the report by Christensen et al.,14 after 1,177 cases of ERCP, the incidence of cardiopulmonary diseases was relatively rare, with heart diseases occurring in 11 cases (0.9%) and pulmonary diseases in 18 cases (1.5%). Arrhythmia and ischemic heart disease accounted for the greatest proportion of the heart diseases, and the pulmonary diseases were mostly pneumonia and respiratory failure. According to the study of Fisher et al.,13 ERCP is commonly associated with clear hematological changes, hypoxia, and myocardial ischemia. However, the frequency and severity of ERCP-related cardiopulmonary diseases were not significantly different between patients older and younger than 65 years. Patients with myocardial infarction or coronary artery disease also showed a similar difference. Post-ERCP myocardial damage was not associated with the type of anesthesia, comorbidity, or the risk of cardiopulmonary diseases. Therefore, old age or cardiopulmonary disease is not an absolute contraindication.
The most commonly encountered issue during a therapeutic ERCP in patients with severe cardiovascular disease is the risk of hemorrhage from the use of anticoagulants and/or antiplatelet agents. Diagnostic ERCP without endoscopic sphincterotomy (EST), in patients using an anticoagulant for cardiopulmonary disease, is a low-risk procedure that does not further increase the risk of hemorrhage. Hemorrhage occurs in approximately 0.3% to 2% after EST, and discontinuing aspirin or nonsteroidal anti-inflammatory drugs for about a week before the procedure does not further reduce periprocedural bleeding. On the contrary, warfarin or heparin significantly increases the risk of hemorrhage when administered within 3 days after EST.2,3 It is therefore recommended to discontinue warfarin 3 to 5 days before a high-risk procedure in high-risk patients, and to resort to a "bridging anticoagulant therapy" by using heparin or low molecular weight heparin (LM-WH), which should be discontinued 4 to 6 or 8 hours, respectively, before the procedure and restarted 6 to 8 hours after the procedure, if there is no bleeding. Warfarin can be administered again from the evening of the procedure, and it is recommended to use LMWH until the international normalized ratio is recovered to an appropriate level. Antiplatelet drugs should be discontinued and replaced with aspirin 7 to 10 days before the procedure, after consulting with a cardiologist, when a drug-eluting stent had been inserted for >12 months or when an uncovered stent was used. If the procedure is necessary, antiplatelet drugs can be discontinued temporarily and then restarted from the day after the procedure if a drug-eluting stent had been in place for >6 months. If antiplatelet therapy could not be discontinued in case of emergency or should be restarted early, the clinician should consider selecting an endoscopic procedure with minimal risk of bleeding, or switching to another drug as a bridge therapy. A local hemostatic procedure should be available, and used if necessary, during a procedure. Moreover, use of drug antagonists that inhibit antithrombotic activity, or transfusion should be considered carefully.
Precautions for endoscopic sedation
Cardiopulmonary complications from endoscopy under conscious sedation accounts for about 40% of the overall adverse effects, occurring in an average of 2 to 5.4 of 1,000 cases, and mortality, which reaches 0.3 to 0.5 of 1,000 cases.13,14,15 Conscious sedation for endoscopy should be performed carefully in patients aged 70 years and older; such patients account for 30% of the overall patients reported to experience an adverse effect. Among 6,092 ERCP cases performed under sedation, cardiopulmonary complications were reported in 2.1%, with the incidence ranging between 1.13% and 2.4% during the ERCP procedure.15 The American Society of Anesthesia (ASA) categorized the risks of sedation and anesthesia into five categories according to the patient's physical status. Patients in physical status I, II, or III are capable of receiving endoscopic sedation performed by an endoscopist or a trained nurse without an anesthesiologist's help.16 However, physical status IV and V mostly require preforming the procedure under general anesthesia, and an anesthesiologist should be in charge of the sleep induction and sedation of the patient. In Korea, most endoscopies performed under conscious sedation, including ERCP, are mostly done by endoscopists or specially trained nurses. Anesthesiologist-directed sedation is now done in only a few hospitals.
Older patients are more responsive to sedative-hypnotics for conscious endoscopic sedation. Older patients usually have less muscle and more fat relative to the body mass, and this delays the metabolism of fat-soluble benzodiazepine and, in turn, markedly increases the clinical effect of the drug. Lower renal and hepatic functions also reduce drug metabolism, which is why older patients take more time to recover from medication. Increased sensitivity of the central nervous system to sedative-hypnotics, change in drug receptors, and increased cumulative dose in the body result in the reduction of the drug dose required for sedation. In other words, cardiopulmonary complications are induced quite easily in older patients even when a standard dose of sedative-hypnotic is used. Therefore, sedatives for older patients should have as short a half-life as possible, with a small dose size for slow titration, and a minimal cumulative dose should be used.17,18 Propofol, which has a short safety margin, should be used with care in older patients; however, recent studies reported that propofol could also be safely used in older patients. It would still be advisable; however, to start gradually from half of the dose administered in healthy adults. The common adverse effects of propofol are reduced vasoconstriction of the blood vessels supplying the heart, thereby lowering the cardiac output, systemic vascular resistance and arterial pressure, and respiratory inhibition, which can be improved rapidly once the intravenous injection is discontinued. One limitation, however, is that there is no available propofol antagonist yet. During endoscopic sedation, decreased oxygen saturation is observed in about 40% to 70% and severe hypoxia (oxygen saturation ≤85%) in about 15%, both of which are observable in patients with multiple comorbidities or in older patients. Hypoxia occurs frequently in older patients with heart or pulmonary disease, in close association with arrhythmia or ST-T changes.18 Opioids exert analgesic and sedative actions by combining with specific receptors present in the central nervous system and peripheral tissues, and each of these drugs has a different pharmacokinetic range and analgesic effect depending on its chemical structure. Fentanyl, with a more rapid onset time and shorter half-life, would be more appropriate for older patients than meperidine. In addition, when combined with a monoamine oxidase inhibitor, fentanyl does not create serious drug interactions and is less associated with cardiovascular adverse effects. For intravenous injection, 50 to 100 µg is initially administered and then 25 µg every 2 to 5 minutes until achieving a proper sedation. The dose should be reduced by >50% in patients aged 60 years or older.17
Common sedatives and analgesics are not absolutely contraindicated in old patients or those with severe condition. In older patients with cardiopulmonary disease, it is recommended to provide oxygen along with pulse oximetry, electrocardiography monitoring, and blood pressure and pulse rate measurements to avoid the risk of hypoxia. In patients with chronic obstructive pulmonary disease, the possibility of decreased oxygen saturation and CO2 retention may be identified in advance by using capnography; however, capnography equipment is rarely distributed in Korea. It is advisable to refer to an anesthesiologist when endoscopic sedation is necessary in patients classified as having ASA physical status IV with a severe systemic disease that is a constant threat to life, such as severe congestive heart failure and end-phase renal failure, or those in physical status V with a risk of death within the next 24 hours. Ultimately, endoscopic sedation-related complications may be predicted and minimized only by understanding the right dose and dosage of drugs and conducting proper patient monitoring.
Go to :
PREPARATION OF GUIDEWIRE
The guidewire is an essential accessory in ERCP that functions as a support and guide for accessory replacement or insertion during various procedures, from selective cannulation to stenting, gallstone removal, and histologic tissue acquisition or cytology in the pancreatic duct, bile duct, and intrahepatic bile duct. Many varieties of guidewires are available to choose from according to the operator's preference and type of procedure.
Materials and composition of guidewires
Various types of guidewires for ERCP are commercially available; they are mostly composed of a stiff shaft that can support the passage of various accessories, including a catheter, sphincterotome, drainage tube, balloon dilator, and bougie, and a hydrophilic soft tip that is flexible and smooth, for tracking and entering desired routes. Guidewires are also categorized into monofilament wires, coiled wires, and coated or sheathed wires according to their structure. Monofilament wires are made of stainless steel for solidity. The coiled spring tip provides gradual flexibility and is commonly used as an esophageal bougie. Coiled wires are composed of a monofilament core on the inside and a spiral coil on the outside, providing solidity and flexibility at the same time; this combination enhances its trackability, which is useful for the handling of tissues in a particularly crooked stricture area. Most coiled wires are coated with Teflon for less resistance. Similarly, coated or sheathed wires are composed of a monofilament core covered with Teflon, polyurethane, or other polymer sheath. The monofilament core on the inside is made of stainless steel, nitinol, or shape memory alloy. The sheath has radiolucency, smoothness, and insulation improved by changing its chemical profile and structure.19 Most ERCP guidewires commonly used in Korea, including Jagwire, Hydra (Boston Scientific, Natick, MA, USA), Tracer (Cook Endoscopy, Winston-Salem, NC, USA), and Visiglide guidewire 0.025 in (Olympus Medical System, Tokyo, Japan) have a nitinol core covered with Teflon or polytetrafluoroethylene sheath. These guidewires are composed of a smooth, hydrophilic tip and a supporting shaft below. The tips may be straight, angled, J shaped, or tapered-it is difficult to tell which is the best type; however, clinicians may select one of them according to the clinical purpose, such as cannulation of the ampulla of Vater, insertion into the intrahepatic bile duct, or passage through a stricture. The type of sphincterotomes and coordination with the catheter may be more important than the guidewire alone in these situations.
The length of a guidewire ranges between 150 and 650 cm; however, guidewires of around 450 cm are the most commonly used. The operator alone cannot handle this long length and therefore requires the support of an assistant. Recently, a short guidewire system was developed by which the operator can fix and handle a 260-cm guidewire with an endoscope, without any help from an assistant. This system requires less time for inserting a second guidewire or replacing a guidewire, and less help from an assistant; however, it is still not popular in Korea and should be supported by more results in a larger population of patients.
The diameter of a guidewire ranges between 0.46 and 0.97 mm (0.018 to 0.038 in); however, guidewires of 0.018, 0.025, and 0.035 in, particularly 0.035 in, are commonly used.19 The newly introduced Visiglide guidewire 0.025 in has the same stiffness as the 0.035-in guidewires. A guidewire with a diameter of 0.018 in is often used for insertion of a 3-Fr pancreatic duct stent; however, it is too thin to support itself and may be difficult to fix with an elevator, inducing a difference in the level of difficulty depending on the operator.
Clinical usefulness of guidewires
As an ERCP guidewire functions as a support during catheter replacement, stenting, and histological test, maintaining the guidewire is important for a successful procedure. The choice of the appropriate guidewire may change according to the type of procedure or the preference of the endoscopist. The basic characteristics of the commonly used guidewires are described in Table 1. In addition, reports have suggested that the success rate of selective biliary cannulation could be increased and the frequency or severity of post-ERCP pancreatitis could be reduced by using a sphincterotome equipped with a guidewire, compared with the conventional application of contrast medium for selective cannulation.20,21,22,23,24,25,26,27 Whether it actually reduces the frequency of post-ERCP pancreatitis is still controversial. However, complications were not further increased in most cases, and the increased success rate of selective cannulation and the reduced procedural time corroborate the role of the guidewire for selective cannulation in the early phase of the procedure, rather than just being a support device. Two previous meta-analysis studies showed that primary wire-guided cannulation increases the primary cannulation rate and reduces the risk of post-ERCP pancreatitis compared with the standard contrast injection method.28,29 Also, a recent review of 12 randomized controlled trials by Tse et al.30 showed that guidewire-assisted biliary annulation seems to be the most appropriate first-line cannulation technique. Compared with the contrast-assisted cannulation technique, the guidewire-assisted cannulation technique increases the primary cannulation rate and reduces the risk of post-ERCP pancreatitis.
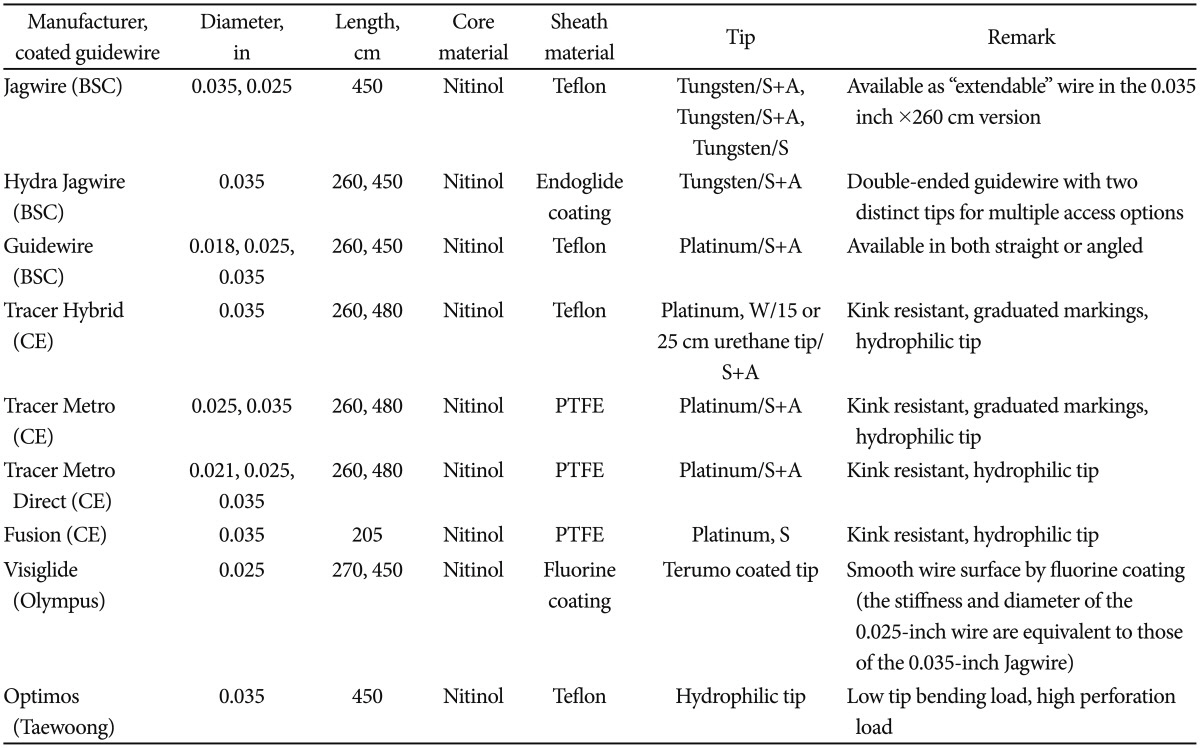
Table 1
Baseline Characteristics and Details of the Commonly Used Guidewires in Korea
Modified from Somogyi et al. Gastrointest Endosc 2007;65:571-576, with permission from Elsevier.19
BSC, Boston Scientific; CE, Cook Endoscopy; PTFE, polytetrafluoroethylene; S, straight; A, angled; C, curved.
![]()
Guidewire-related complications
As guidewire tips are usually smooth and hydrophilic, only a few complications have been reported thus far. The common risk factors of perforation are anatomical changes from factors such as Billroth II subtotal gastrectomy, EST and precut sphincterotomy, intramucosal injection of contrast agent, long procedure time, periampullary diverticulum, bile duct stricture, SOD, old age, and an inexperienced operator.2,3 Guidewire-related perforation often occurs locally around the ampulla of Vater, or proximal biliary obstruction occurs in the presence of these risk factors. Perforation occurs from forcing the entry of a guidewire when biliary cannulation is difficult; the risk of perforation may be increased when there is ampullary edema or inflammation from repeated attempts of cannulation. There is a possibility, therefore, that perforation occurs as a result of using a guidewire as a rescue method after multiple attempts of selective biliary cannulation.31 Inexperienced operators or assistants could also cause perforation injuries. Some may not detect a microperforation created by the guidewire and still insert a drainage tube or dilatator, further increasing the size of the perforation to the extent of requiring a surgery. In terms of instruments, perforation may be also associated with the texture of the guidewire itself, the flexibility of the tip, or the nature of the instrument itself.32,33
Guidewire-related perforations are initially asymptomatic in case of retroperitoneal microperforation, and may develop into fever or abdominal pain when early detection is delayed. However, mild abdominal pain is the only clinical symptom that presents in most cases; fever, leukocytosis, or peritonitis occurs rarely and improves quite rapidly. As most cases are local and rarely as deep as the retroperitoneum, patients usually recover within 24 to 48 hours after conservative treatments involving fasting and broad-spectrum antibiotics. Nasogastric intubation is unnecessary in most cases. Biliary drainage or repeat ERCP for biliary stenting may be attempted in case of proximal bile duct perforation due to severe biliary stricture.32,33
Go to :
CONCLUSIONS
Safe and effective ERCP can be ensured by the proper performance of the designated roles of the operator and assistants. An optimal space and appropriate endoscopic sedation are also essential factors for a safe and successful ERCP. Clinicians need to understand the patient's condition before the procedure to minimize the risk of complications. With the recent population aging and increased prevalence of cardiopulmonary diseases, it is no longer necessary to delay therapeutic ERCP in older persons and patients with cardiovascular diseases for fear of ERCP-related complications. However, ERCP is an invasive procedure with a high frequency of cardiopulmonary diseases and other complications among the gastrointestinal endoscopies. MRCP or EUS should be considered first before conducting a diagnostic ERCP. In super-aged persons with the risk of complications or in high-risk patients with severe cardiopulmonary disease, therapeutic ERCP should be conducted rapidly and accurately, with sufficient pretreatment, by an experienced endoscopist. During endoscopic sedation, the risk of complications should be minimized by applying enough monitoring during the procedure and recovery periods so that any adverse event could be detected early. Finally, the use of a guidewire is essential in most cases but requires cooperation with assistants. It is also worth considering as the initial cannulation method to increase the success rate of selective cannulation and decrease the severity or frequency of post-ERCP pancreatitis.
Go to :
 XML Download
XML Download