

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Situs inversus is a congenital condition in which the major organs within the abdomen or the thoracic cavities are reversed from their normal positions. Situs inversus totalis (SIT) is a rare condition in which the abdominal and thoracic organs are completely reversed. Its incidence is approximately one in every 10,000 to 50,000 live births. Although the exact cause is unknown, SIT generally does not cause inconvenience in daily life. SIT has no pathophysiological significance, and the survival rate of patients with SIT does not differ from that of healthy persons.1,2 However, patients with SIT require a thorough radiological examination to identify the presence of associated variations before undergoing invasive procedures such as surgery or hemostasis of gastrointestinal hemorrhage because they may have an abnormal spleen or other abnormalities in anatomic structures3,4 along with reversed organs.5
Percutaneous endoscopic gastrostomy (PEG) is one of the most frequently performed enteral feeding methods for patients with dysphagia and a normal gastrointestinal function, and is generally highly successful, with a low death rate. This procedure can be easily implemented in patients with serious underlying diseases.6 The reported complications are surgical site infection, bleeding, gastrocolic fistula, and displacement of the feeding tube. In severe cases, more critical and life-threatening complications are seen, including aspiration pneumonia, intestinal perforation, peritonitis, and necrotizing fasciitis, requiring extracaution during the procedure.7 In particular, caution should be exercised concerning the differences in anatomical location when performing PEG on a patient with SIT.
Here, we report the case of a patient with SIT who underwent a PEG procedure because of dysphagia because of intracerebral hemorrhage (ICH), and include a review of the literature.
Go to : 
CASE REPORT
A 65-year-old woman was transferred to our department for PEG insertion during nasogastric tube feeding because of dysphagia caused by ICH. She was taking medication for hypertension and osteoporosis for the last 7 years. She was diagnosed with SIT during a colonoscopy performed 2 years prior; she has no family history of this condition. At the time of transfer, she was maintaining a blood pressure of 130/80 mm Hg, heart rate of 65 to 80 beats per minute, body temperature of 36.5℃, and respiratory rate of 18 breaths per minute with alert consciousness. Her heart rate was normal without heart murmur. No difference was found from the previous examination of the chest, and no abnormal findings were detected in the abdomen, limbs, and skin. Analysis of peripheral blood showed a white blood cell count, platelet count, and hemoglobin of 5,170/mm3, 9.7 g/dL, and 290,000/mm3, respectively.
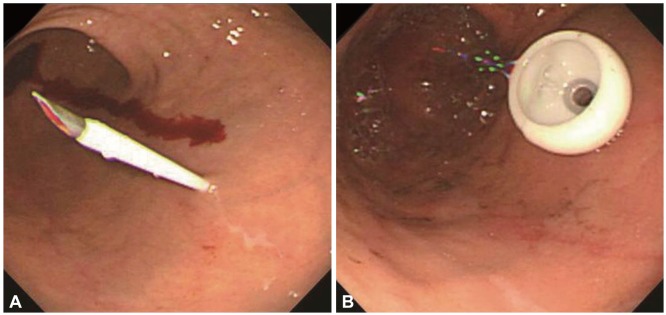
The liver function test results were as follows: aspartate aminotransferase/alanine aminotransferase, 13/9 IU/L; prothrombin time-international normalized ratio, 1.08; and partial thromboplastin time, 32.4 seconds (reference range, 20 to 38). The renal function tests were within the reference ranges. Dextrocardia was observed on a chest radiograph (Fig. 1), and complete right to left reversal of internal organs was detected on abdominal computed tomography (CT) scan, indicating a finding of SIT (Fig. 2). No abnormal findings were found on the CT scans of the spleen and major blood vessels. Upper gastrointestinal endoscopy was conducted identical to a general endoscopic procedure, with the patient in a left lateral decubitus position. Along with preoperative monitoring of pulse rate and oxygen saturation, midazolam (3 mg) and propofol (50 mg) were administered via intravenous injection as a pretreatment. The endoscope was turned counterclockwise when it was passed from the bulb to the descending part of the duodenum. The gastric angle, when observed with a J shaped retroflection at the antrum, was mirrored from its normal position. No specific findings were detected during the endoscopy except for a mild chronic superficial gastritis. A puncture site was chosen with the help of an endoscopic light after manually pressing the stomach wall to find the thinnest site. Subsequently, a gastrostomy feeding tube (PEG-24-Pull; Wilson-Cook Medical GI Endoscopy, Winston-Salem, NC, USA) was inserted into the anterior wall of the lower gastric body, which looks like the posterior wall of the lower gastric body in a normal person (Fig. 3). The nutrition was delivered directly into the stomach the next morning after PEG insertion, and no specific complications were observed.


Go to :
DISCUSSION
SIT is a rare congenital condition in which the abdominal and thoracic cavity structures are completely opposite of their normal positions. The exact cause of this condition has not been clarified, except for a genetic predisposing factor. According to Layton,8 the allele regulating the asymmetric expression of normal organ placement is a complete dominant one, and the reversal of organ position results from the absence of that allele. A patient with SIT requires a thorough radiological examination to identify the presence of associated anatomic variations before undergoing invasive procedures such as surgery or hemostasis of gastrointestinal hemorrhage because the condition may be associated with an abnormal spleen and other abnormalities in anatomical structures. Lee et al.9 performed endoscopic hemostasis on a SIT patient with Dieulafoy gastric bleeding. However, several attempts with endovascular embolization and hemoclips failed, so they performed a suture and ligation of the Dieulafoy lesion as well as total resection of the accessory spleen with devascularization of prominently developed vessels around the upper stomach. Kang et al.10 reported a case study of an early gastric cancer patient with SIT in whom surgery was completed safely by identifying the anatomic variations of the right gastric artery directly arising from the aorta and the splenic artery directly arising from the celiac artery on a preoperative abdominal CT scan.
PEG insertion is an effective and safe procedure for patients having difficulty in swallowing, with the placement of a feeding tube into the stomach. However, complications continue to be reported despite advancements in the procedure.11 The most common complication of PEG is surgical site infection, followed by gastric bleeding, pneumoperitoneum, displacement of the feeding tube, aspiration pneumonia, intestinal perforation, peritonitis, necrotizing fasciitis, buried bumper syndrome, and others, accounting for 5% to 40% depending on the reports.12 Although PEG insertion is relatively safe and effective, the procedure requires extra caution because minor complications may lead to life-threatening situations due to underlying illnesses in the presence of malnutrition and old age. In particular, when performing PEG in patients with SIT, the procedure requires added caution because of the unfamiliar structures associated with anatomical placement and variations, as well as because of postoperative complications.
Endoscopic retrograde cholangiopancreatography (ERCP) and endoscopy are generally performed in the right lateral decubitus position in patients with SIT, taking into consideration the reversed abdominal organs.13 However, ERCP could also be performed without difficulty in the left lateral decubitus position, according to Chowdhury et al.14 In a previous report, when endoscopy and colonoscopy were carried out in a patient with SIT, with careful preparation and in keeping with the general principles, in the left lateral decubitus position as with ordinary patients, the procedures were successfully performed without pain or complications except for a prolonged examination time.15
In conclusion, PEG insertion was performed in a patient with SIT with the help of an endoscope, by puncturing the anterior wall of the lower gastric body, which looks like the posterior wall of the lower gastric body in a normal person, after identifying the presence of associated anatomic variations. No complications occurred. Although PEG insertion in a patient with SIT may be rare and accompanied by different complications, the procedure could be implemented without difficulty if the anatomic variations as well as the reversed organs in these patients are carefully considered.
Go to :
 XML Download
XML Download