

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In 1969, Brenner et al.1 were the first to describe a case of carcinoid tumor originating within the esophagus. Esophageal carcinoid tumors are thought to arise from the argyrophilic endocrine cells of the mucosa, which were first detected in 1974.2 Esophageal carcinoid tumors remain some of the rarest of all carcinoid tumors, with only several cases previously reported in the literature. Here, we report successful endoscopic mucosal resection (EMR) of a low esophageal carcinoid tumor and review the literature. To our knowledge, there have been no previous case reports of esophageal carcinoid tumors in Korea.
CASE REPORT
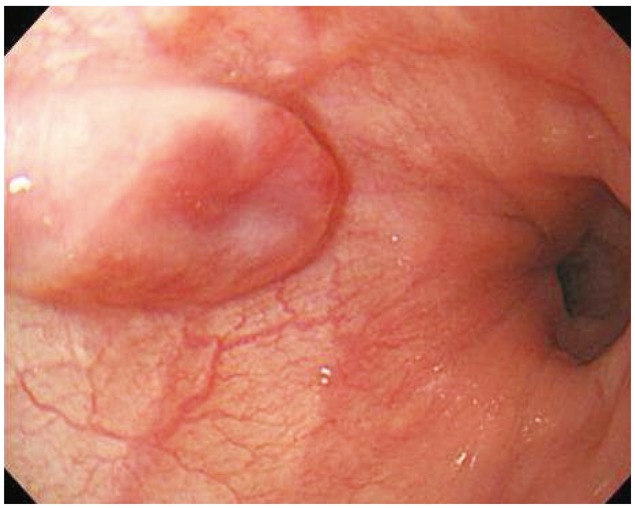
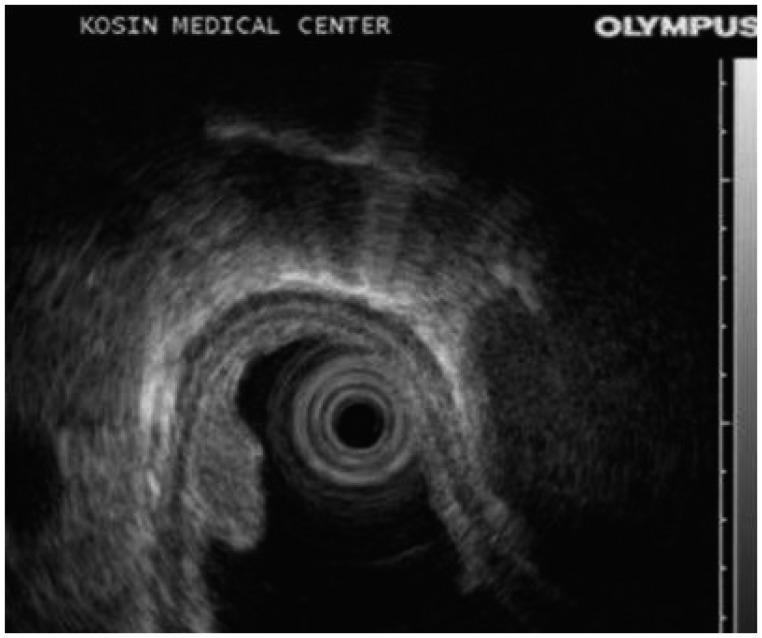
A 49-year-old woman underwent upper endoscopy due to intermittent epigastric soreness and heartburn. A 0.8×0.5-cm, ovoid, elevated, submucosal esophageal lesion was detected 35 cm from the incisors (Fig. 1). The overlying mucosa was intact but showed slightly erythematous central change and had a soft consistency. The surface of the tumor was stained with iodine. Endoscopic ultrasonography (EUS; 20 MHz, miniprobe) demonstrated a 4.4×3.3-mm, well demarcated, homogenous, hypoechoic, round mass lesion within the mucosal layer, and the submucosal layer beneath the lesion was observed to be intact (Fig. 2).
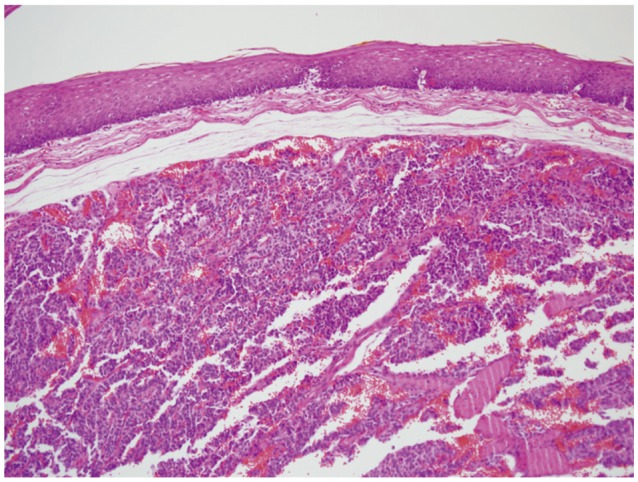
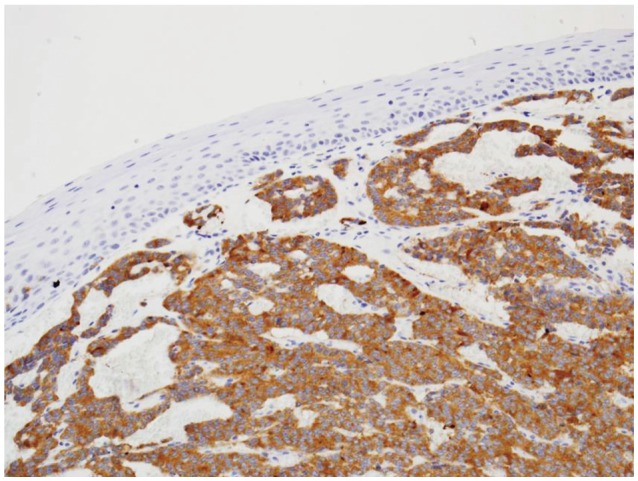
A biopsy was performed and the mass was diagnosed as a carcinoid tumor. We informed the patient of the characteristics of carcinoid tumor. The patient chose to undergo endoscopic resection. EMR was performed by snaring the lesion following a submucosal saline injection (Fig. 3). There were no immediate complications. Histologic examination of the resected specimen revealed that the tumor was located in the mucosal layer (between the mucosa and muscularis mucosa) as indicated by EUS. The tumor consisted of round cells arranged in sheets without mitoses, and the resection margin was free (Fig. 4). Immunohistochemical studies demonstrated positivity for neuron-specific enolase, synaptophysin and chromogranin as supporting evidence of an esophageal carcinoid tumor (Fig. 5). A second endoscopy performed 2 months after the first demonstrated a linear whitish scar, with no residual lesion. Computed tomography imaging of the thorax was unremarkable.
In the present patient, there were no such clinical manifestations.
Lindberg et al.6 reported that esophageal carcinoid tumors exhibit marked male predominance, with a male to female ratio of 6:1. Age at diagnosis is widely variable, ranging from 45 to 82 years. Symptoms presented in their study were dysphagia (64%), weight loss (43%), pain (14%), reflux esophagitis (14%), fatigue (7%), and melanotic stools (7%).6 Only one patient had previously reported symptoms consistent with carcinoid syndrome.7
Klöppel et al.8 reported that most esophageal carcinoid tumors histopathologically are poorly differentiated neuroendocrine carcinomas and mixed endocrine-exocrine carcinomas, usually ranging from 4 to 10 cm in diameter. They present as fungating or ulcerated masses deeply infiltrating into the esophageal wall and are associated with early spread to the regional lymph nodes or infiltration of adjacent organs. In contrast, most well-differentiated neuroendocrine tumor/neuroendocrine carcinomas are less than 4 cm in diameter, present as polypoid lesions and are rarely associated with lymph node metastases and thus have an excellent prognosis.8
The management of locoregional carcinoid tumors depends on tumor site and primary site as well as the general condition of the patient. Resection is the primary treatment approach for most localized carcinoid tumor.9 Most early reports recommend that esophageal carcinoid tumors be treated surgically by esophagogastrectomy or subtotal esophagectomy with gastroesophageal anastomosis.1,10,11 Currently, however, EMR of selected carcinoid tumors is accepted as a safe and effective alternative.12 The use of a ligation band at the lesion base may increase the ease and safety of EMR, and therefore ligation bands have been utilized for the treatment of other esophageal pathologies (i.e., Barrett's dysplasia) and for rectal carcinoid resection.13
EUS allows accurate description of the depth of tumor invasion into the esophageal wall, as well as the identification of internal features of the tumor.14 In our patient, the location of the tumor was clearly demonstrated by EUS and was consistent with pathological findings. EUS appears to be an excellent method to detect the depth of tumor invasion in the esophageal wall and has proven utility in staging and interventional planning (endoscopic or surgical) for gastrointestinal carcinoid tumors.15
Esophageal carcinoid tumors is a very rare disease. However, with increasing rates of screening upper endoscopy and recent technical improvement in endoscopy and radiology, detection of small esophageal carcinoid tumors may be increasing, adding to our findings. Due to improvements in EUS imaging techniques and EMR techniques, endoscopic treatment can successfully achieve complete resection of selected esophageal carcinoid tumors with few complications. We report a case of successful EMR of a low esophageal carcinoid tumor.

 XML Download
XML Download