

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastrointestinal (GI) lipoma is a benign subepithelial tumor predominantly arising in the submucosal layer. It can be found throughout the GI tract, but common sites are the cecum, sigmoid colon, small intestine, and stomach. As most of GI lipomas are small, they are usually asymptomatic and may be accidentally found during endoscopy. However, some of them can produce symptoms, such as abdominal pain, constipation, and intestinal obstruction, according to their location and size. Lipomas in the small intestine may become a lead mass provoking intussusceptions. Intussusceptions are defined as prolapse of one portion of the intestine into an immediately adjacent portion. Although intussusceptions in children are idiopathic and are treated by barium reduction, adult intussusceptions need surgery because of the existence of lead points such as benign tumors, polyps, or carcinomas.1 Recently, due to advanced endoscopic techniques, subepithelial lipomas can be treated by endoscopic procedures such as endoscopic submucosal dissection, unroofing technique, or snare polypectomy.
We report a case of a lipoma arising in the ileum, causing repetitive ileocolic intussusceptions through the ileocecal valve (ICV), which was found during colonoscopy; it had been responsible for the patient's intermittent abdominal pain and weight loss of 15 kg for 2 years, and endoscopic snare polypectomy within the ileum by cap-assisted colonoscopy successfully removed it.
CASE REPORT
A 73-year-old woman presented with intermittent abdominal pain and weight loss of 15 kg for the past 2 years. Her pain was frequently accompanied by nausea and/or diarrhea and tended to be aggravated by food intake. Her past medical and familial histories were unremarkable. On examination, vital signs were stable but she appeared a little chronically ill. Her abdomen was soft with no palpable mass; bowel sounds were somewhat increased and mild tenderness was noted in the right lower quadrant (RLQ). Initial laboratory blood tests were normal.
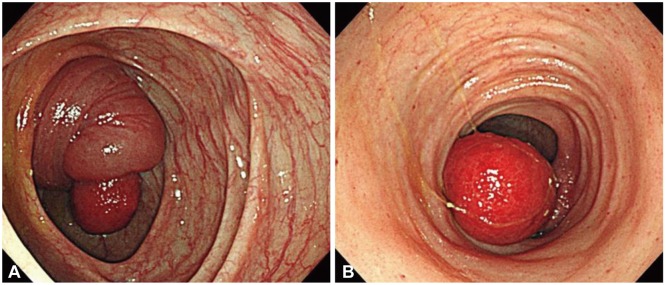
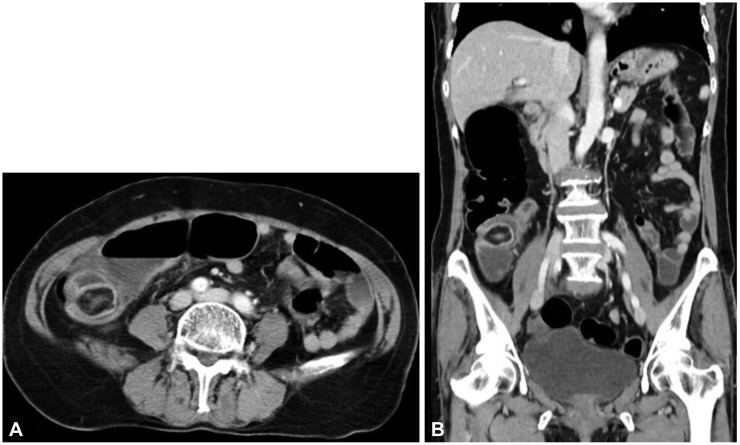
Colonoscopy revealed an erythematous polypoid mass at the proximal ascending colon and it seemed to have a huge stalk thicker than the mass itself (Fig. 1A). With air being inflated during colonoscopy, it was not seen in the colonic lumen and abruptly disappeared. As the endoscope was advanced through the ICV, there was a polypoid mass in the terminal ileum and multiple tiny hemorrhagic spots on the ileal mucosa; the mass intussuscepted into the colon through the ICV had reverted back to its original site in the terminal ileum (Fig. 1B). The thick stalk must have been an intussusceptum of the terminal ileum with the mass as a lead point. In its original position in the ileum, a short stalk was identified on the base of the polypoid mass. Additionally, abdominal computed tomography (CT) scan revealed a well-demarcated pedunculated subepithelial mass with fat attenuation indicating a lipoma of the terminal ileum (Fig. 2).
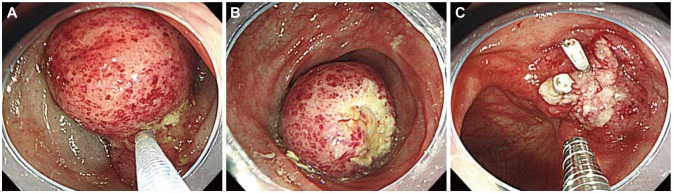
This ileal lipoma was thought to have been responsible for her abdominal pain and weight loss on account of repeated ileocolic intussusceptions causing intermittent intestinal obstructions. Because the patient strongly refused surgical treatment, we planned to endoscopically remove her ileal lipoma considering potential sequelae of ileal resection. In order to perform endoscopic procedure in the spacious colonic lumen, we tried to retract the mass into the colonic lumen through the ICV but unfortunately failed. Therefore, to keep a clear visual field within the narrow lumen of the ileum, a cap-assisted colonoscopy technique was used. After submucosal injection into the base of the mass, a snare polypectomy was performed within the ileum (Fig. 3A, B). And then, three clips were placed to prevent delayed hemorrhage or perforation (Fig. 3C). There were no immediate complications after the polypectomy. The histopathology report confirmed a 2.6×2.7 cm subepithelial lipoma. At 2 days of fasting after the procedure, oral intake was started and the patient complained of no symptoms related to food intake. Since resection of the lipoma, her body weight has gradually restored.
DISCUSSION
The lipoma of this patient was accidentally found during colonoscopy to evaluate causes of chronic abdominal pain and weight loss. If her ileal lipoma had not been found as ileocolic intussuception during endoscopy, we could not have considered the lipoma as a cause of her symptoms. Repeated ileocolic intussusceptions due to the large lipoma of the ileum had provoked her abdominal pain characterized by meal-induced symptom aggravation. If endoscopic resection had failed or not even been tried, this 73-year-old woman would have had to undergo surgery and might have been complicated by surgical sequelae including absorption disorder. However, as the patient refused surgery and accepted possible complications of endoscopic treatment, her ileal lipoma could be endoscopically removed with great success and no complications, and subsequently her symptoms disappeared.
In the small intestine, benign tumors are relatively common compared with malignancy. They include leiomyoma, adenoma, lipoma, hemangioma, and hamartoma, of which lipoma is the third most common. The terminal ileum is the most frequently affected site of small intestinal lipomas. They are solitary rather than multiple and originate predominantly in the submucosal layer, except for 10% in the serosal layer.2,3 Symptoms of small intestinal lipomas depend on the lipoma's location and size. It was reported that intestinal lipomas larger than 2 cm in size cause symptoms such as abdominal pain, nausea, diarrhea, or abdominal masses and some in the RLQ of the abdomen can mimic acute appendicitis.4 In addition, adult intussusceptions have been reported to usually present with chronic and partial intestinal obstruction.5 In our patient, intermittent ileocolic intussusceptions by the ileal lipoma as a lead point were responsible for chronic abdominal pain and weight loss.
Abdominal CT is the most accurate diagnostic modality of intestinal lipomas by showing a smooth well-circumscribed unhomogeneous soft tissue mass of fat density (Housefield unit between -80 and -120).6 Endoscopic findings are usually polypoid subepithelial tumors with yellow to red-appearing mucosal surface. In our patient endoscopy accidentally captured the unique image of the ileocolic intussuseptions by the ileal lipoma and, furthermore, that image was sufficient to explain the chronic and recurrent feature of the patient's symptoms.
Ileal lipomas do not have malignant potential and, therefore, removal is not necessary. However, complications, such as hemorrhage, obstruction or intussusceptions as in our patient, may require their removal. Although such cases had traditionally been treated by surgery, endoscopic removal has been increasingly reported with the advances in endoscopic procedure.7,8 Endoloop ligation, endoscopic submucosal dissection and unroofing technique are recently reported for such endoscopic procedures. Unroofing technique is a procedure where lipoma is spontaneously emitted from the exposed mucosal surface after incision of the upper half of the mucosal surface of the subepithelial mass. This technique could reduce the risk of hemorrhage and perforation in resecting subepithelial mass. Another effective and safe procedure is to use a detachable snare, the endoloop, which enables slow mechanical transaction and reduces risks of hemorrhage and perforation. A large colonic lipoma of >5 cm in size was reported to be safely removed by snare polypectomy after stepwise reduction in size by using both unroofing and endoloop techniques.9 However, unroofing or endoloop technique takes time for a mass to be completely removed. Considering that the large lipoma remained in the narrow ileum might produce any unexpected complications, we determined to avoid its delayed removal and therefore to perform snare polypectomy.
Although snare polypectomy could be performed for small lesions, particularly pedunclated or narrow-based lesion, within the terminal ileum according to the same principles as in the colon, endoscopic procedure in a narrow lumen of the small intestine is more difficult than in the colon and has high risk of bowel perforation. Also in performing snare polypectomy in the terminal ileum, endoscopic operation is impeded by a large mass in the narrow space and the approach to an appropriate injection site may be difficult. Numerous villi in the ileum make submucosal injection site not as distinguishable as in the colon. Therefore, submucosal injection for lifting a tumor may be excessively injected and makes the narrow lumen narrower due to the lifted tumor. It was reported that endoscopic treatment of an ileal lipoma could be performed in the colonic lumen after bringing it into the colonic lumen by aspiration.7 Taken together, we also tried to aspirate the tumor into the spacious colonic lumen, but several trials ended up with failure. Attaching a transparent cap to the tip of a colonoscope can provide an advantage: cap-assisted colonoscopy keeps a distance appropriate for a clear visual field. With this technique, we could safely perform snare polypectomy of a relatively large ileal lipoma within the ileum.
This case demonstrates that an ileal lipoma can cause significant weight loss due to repetitive ileocolic intussusceptions accompanied by abdominal pain. Although indications of snare polypectomy in the ileum have not yet been established, we can speculate from our experience in the case that a large ileal lipoma adjacent to the ICV, with any stalk and not having broad base, could be removed with snare polypectomy by cap-assisted colonoscopy. The present case suggests that snare polypectomy by cap-assisted colonoscopy may be an alternative to surgery for resecting a symptomatic benign tumor in the ileum.
 XML Download
XML Download