

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of colorectal cancer is increasing rapidly in South Korea, taking up a significant position in the viewpoint of public health. The incidence, however, can be effectively reduced by removing colon polyps, the preceding lesion of co-lorectal cancer.1,2 Academic bodies in the field of gastroenterology have published screening guidelines to detect colorectal cancer and colon polyps in their early stage so as to reduce the mortality associated with advanced colorectal cancer.3,4 The most common method of removing colon polyps is endoscopic resection, such as snare resection, among others, with or without fluid injection into the submucosal layer beneath colon polyps, as well as hot biopsy and endoscopic submucosal dissection. Endoscopic resection may cause complications such as bleeding, however. Such bleeding after the snare resection of colon polyp may be classified into an immediate bleeding or a delayed bleeding. Generally, the former refers to the bleeding on the cut surface occurring right after the polyp resection, the later occurring after completing the endoscopic resection with the withdrawal of colonoscope. The incidence of immediate postpolypectomy bleeding (IPPB) is reported around 2.1% to 9%,5-8 and resection of large polyp, use of cutting current, or resection of pedunculated polyp are reported as risk factors.8,9
Pedunculated polyps have feeding artery running through the pedicle (stalk). IPPB may be preventable, even without applying adequate current enough to coagulate the artery in the stalk, if the stalk was clipped before the snare resection. But there are few well-structured study evaluating the availability of clipping for preventing IPPB after snare resection of pedunculated polyps, except for sporadic empirical case studies.10 The aim of this study was to evaluate if clipping a stalk of pedunculated polyp before the snare resection is feasible for preventing IPPB.
MATERIALS AND METHODS
Subjects
This multicenter, prospective, pilot study was performed between June 2009 and June 2010, to obtain basic data on the availability of clipping for the prevention of IPPB after the snare resection of pedunculated polyps. Four centers including Asan Medical Center, Chonnam National University Me-dical School, Ajou University School of Medicine and Pusan National University School of Medicine participated in the study. Patients undergoing endoscopic resection of pedunculated polyp with distinct stalk were included in the study, if 1) the size of the pedunculated polyp head is ≥10 mm; 2) the diameter of the stalk is ≥5 mm; and 3) the length of the stalk is ≥5 mm. The size of the polyp head and the diameter and length of the stalk were measured by endoscopists using an 8-mm open forceps in width. Patients with medical or surgical condition unsuitable for colonoscopy or with bleeding tendency due to underlying illness or anticoagulant use were excluded from the study. All patients provided written informed consent.
Clipping and snare resection
Snare resection was performed as follows after clipping pedunculated polyps (Figs. 1-3). First, we made it a general rule to clip perpendicular to the long axis between the middle and the highest tertile of a stalk. When most of the girth was not covered with the first clip, a second was added to the opposite side, or more clips until most of the girth was covered. When deemed most of the girth was clipped, snare was inserted through the working channel of the endoscope, to grab in the middle between the clipping and the site where the pedunculated polyp head and stalk meets. Then the pedunculated polyp was resected with current transmission. The resected polyp was collected for histopathological evaluation. The pedunculated polyp's location and the size of the head were recorded. The procedure was performed by endoscopists with more than 500 cases of experience in colonoscopic polypectomy.
We observed whether IPPB occurred or not. IPPB was defined when there was oozing bleeding on the cut surface, immediately after the polyp resection, which lasts for more than 30 seconds without specific care, or when there was pulsating bleeding on the cut surface immediately after the polyp resection. Occurrence of other complications such as delayed postpolypectomy bleeding (DPPB) or perforation was also observed. DPPB was defined when hematochezia or melena requiring transfusion occurred after withdrawal of the endoscope, when sigmoidoscopy or colonoscopy was performed for the clinical needs, when surgery was required, or when the hemoglobin level was decreased by ≥2 g/dL.
Statistical analysis
For descriptive statistics, 2 or more pedunculated polyps resected in the same patient were treated as separate cases for each polyp. The results were presented as mean±standard deviation, and ranges when necessary. This study was approved by the Institutional Review Boards of each 4 participating centers.
RESULTS
Baseline characteristics of the subjects and polyps
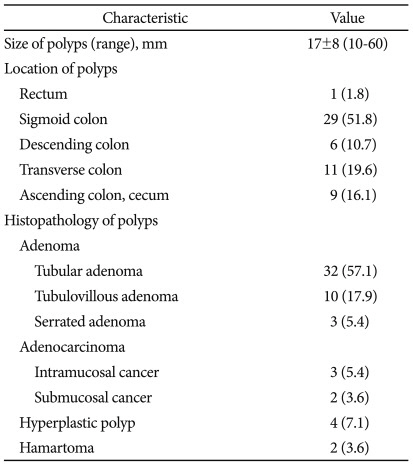
Fifty-six pedunculated polyps detected from 47 patients were registered in the study. The numbers of male and female patients were 36 and 11, respectively; their age was 56±11 years. The size of the patients pedunculated polyp heads was 17±36. The most common location of the pedunculated polyps was the sigmoid colon in 29 cases, followed by transverse colon, ascending colon and cecum, descending colon, and rectum. The most common histopathological finding of the resected pedunculated polyps was tubular adenoma in 32 cases, followed by tubulovillous adenoma and hyperplastic polyp. Baseline characteristics of the evaluated polyps are summarized in Table 1.
Results of snare resection after clipping
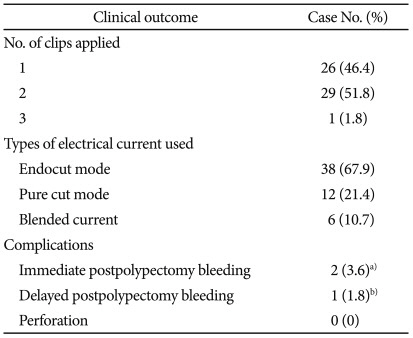
Clipping the adequate site of the pedunculated polyp stalk was successful in all 56 cases. Snare resection after clipping enabled successful en bloc resection in all 56 cases. The number of clips used before snare resection for IPPB prevention was 2.0±0.5 (range, 1 to 3). The most frequently used mode of current for snare resection was the endocut mode of electrosurgical unit made by ERBE (Tübingen, Germany) in 38 cases, in addition to pure cut mode and blended mode.
IPPB after the snare resection occurred in 2 cases (3.6%); one of them a tubular adenoma 25 mm in size found in the descending colon, and another case a tubular adenoma 15 mm in size found in the ascending colon, and both of which showed oozing bleeding. Hemostasis was available in these 2 cases by adding 1 and 2 clips, respectively, to the cut surface. DPPB occurred in 1 case (1.6%) with pedunculated polyp 20 mm in size found in the ascending colon. The patient visited 4 days after the resection due to the hematochezia, and the endoscopy revealed ulcer and exposed vessel at the previous resection site, of which hemostasis was achieved using 5 clips. After that, the patient was improved with conservative management without re-bleeding. No perforation was observed. The results of the snare resection after clipping are summarized in Table 2.
DISCUSSION
In this multicenter pilot study evaluating the availability of clipping for the prevention of IPPB after snare resection of pedunculated polyp, average 2 clips were sufficient to reduce the incidence of IPPB to a relatively low 3.6%. The frequency of IPPB after endoscopic resection of colon polyp is reported around 2.1% to 9%.5-8 Since pedunculated polyp has higher risk of IPPB,8,9 based on previous studies,5-9 it can be speculated that resection of pedunculated polyp without a preventive measure my lead to approximately 9% of IPPB frequency. Therefore, the findings of this study indicate that clipping before resecting pedunculated polyp may lower the frequency of IPPB. IPPB, occurring after endoscopic resection of colon polyp, blurs the endoscopic view for resection interfering safe procedure, prolongs the duration of the procedure, and requires additional endoscopic hemostasis, such as clipping or epinephrine injection, or angiographic embolization. Additional or prolonged hospitalization might be also necessary. IPPB after endoscopic resection not only increases the duration of the procedure, incidence of complications and the need for transfusion, it also may be a risk factor of DPPB.8 Thus, effective prevention of IPPB is very important in terms of safe procedure. Since this study was a pilot study without a control group, further randomized controlled study may be necessary to confirm the effect of clipping.
Preventive measures of IPPB after the high risk pedunculated polyp resection were examined in various studies. Epinephrine-saline mixture injected to the stalk of pedunculated polyp induced mechanical compression of the feeding vessel in the stalk by the fluid and vasoconstrictive effect by epinephrine, reducing the IPPB risk after snare resection of the stalk. This method, however, gave rise to early bleeding within 24 hours after the resection and there are reports of IPPB risk as high as 1.8% to 9.3%, suggesting the effect is not flawless.11-13 Snare resection of the stalk using a detachable snare with or without the injection of the epinephrine-saline mixture were also evaluated in 2 prospective comparative studies, which showed relatively low (1.2%) early and immediate bleeding risk.12,13 This method, however, is not technically easy to place the detachable snare on the adequate site when the size of the pedunculated polyp head is big, and sometimes the detachable snare gets entangled with the snare for resection, causing failure in 5.7% to 15.1% of cases,13-15 which is why we need a more effective method. The clipping method used in this study did not cause any technical failure with relatively low IPPB frequency (3.6%), suggesting that the snare resection of pedunculated polyp after clipping may be an effective, readily available method in clinical practice. Since this was not a randomized comparative study with the previous methods, it was difficult to evaluate its superiority compared to the previous methods.
There were 2 cases of IPPB despite clipping in this study, but we could not find a definite cause of these bleeding. In a study using detachable snare for resection of a thin (<4 mm) stalk reported the occurrence of IPPB in some cases when the thin stalk was cut by the tightened snare.15 But clips hardly cut a stalk, and IPPB cases in this study might have been caused by insufficient compression of the feeding vessel because the clips could not cover the entire girth of the stalk. This implies that the clips should be placed on an adequate location to sufficently cover the girth of a stalk.
There was no perforation in this study, but 1 case (1.6%) of DPPB was observed. In a study using detachable snare to prevent IPPB, 2 out of 28 caess (7.1%) resulted in DPPB 6 and 7 days after the procedure, respectively, when the detachable snare was dislocated.15 Generally, it is assumed that the inflammation on the site of resection and the site held by a detachable snare or a clip becomes fibrotic during healing process, lowering he risk of DPPB. But the risk of DPPB increases when the detachable snare or the clip was dislocated before the vessel was coagulated and the surrounding tissues became fibrotic. It is important, therefore, to make sure the detachable snare or the clip hold a stalk enough and resection should be performed slightly above the detachable snare or the clip so as not to cause a dislocation and lower the risk of DPPB. The frequency of DPPB of this study (1.6%) seems comparable to the level reported in the previous studies after polypectomy (range, 0.3% to 6.1%).16,17 As mentioned above, placing a clip on the adequate location might lower the frequency of DPPB compared to the previously reported level after the snare resection. This hypothesis needs to be confirmed by a clinical study that examines the location of detachable snare or clipping as well as the location of the stalk resection, which could be the basis of establishing a pertinent method of procedure for the prevention of DPPB.
This study has several limitations. First, as mentioned earlier, this is not a comparative study with a control group, making it difficult to draw a definite conclusion on the availability of the clipping, although we have come up with several assumptions. Second, we could not adjust for potential confounding variables such as the diversity of current modes, being a pilot study with relatively small number of patients, or the risk of bleeding due to drug use, for not investigating the exact data on drug use, such as aspirin or non-aspirin antiplatelet agents, and their doses, except for patients using anticoagulants. Third, there was no randomized comparison with the previous procedures, which is why we could not directly confirm whether the investigated method was superior to the previous methods in terms of IPPB prevention and duration or easiness of the procedure. While there have been some ca-ses reporting failure with the previous methods using detachable snare, there was not a technical failure using the snare resection after clipping in this study, reflecting that the pro-cedure is not technically difficult to perform. Also the fact that unlike the epinephrine injection-resection method reporting 1.8% to 9.3% frequency of early and immediate blee-ding, the IPPB frequency in this study was 3.6%, although being an indirect comparison, suggests that this method may not be inferior to the previous methods in terms of efficacy.11-13
In conclusion, the findings of this study is significant in that they provided the basic data suggesting that snare resection after clipping might be an easy and effective procedure for prevention of IPPB after pedunculated polyp resection. Larger controlled comparative studies and direct comparison with the previous procedures as well as prospective studies evaluating the cost-effectiveness of this procedure should be performed in the future to provide a guideline on clipping.



 XML Download
XML Download