

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Synovial sarcoma is a rare type of soft tissue sarcoma that occurs most commonly in young adults.1 It can be found in almost any part of the body, but the most common location is the lower extremity, followed by the upper extremity, trunk, abdomen, and head and neck.2 Retroperitoneal synovial sarcoma, which is the topic of our present case, is a rare finding and represents about 1% of retroperitoneal tumors.3 Since the first report by Pack and Tabah4 in 1954, there have been about 32 cases of retroperitoneal synovial sarcomas. Early detection of retroperitoneal synovial sarcoma is difficult because the retroperitoneal space is highly expandable and deeply hidden. This specific tumor has no special features that would distinguish it from other abdominal and retroperitoneal tumors.5
Recently, we experienced a rare case of retroperitoneal synovial sarcoma presented with obstructive jaundice. Such kind of presentation has never been reported in the previous literature. To the best of our knowledge, ours is the first report on the case of retroperitoneal synovial sarcoma manifested by obstructive jaundice.
Go to : 
CASE REPORT
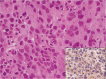
A 78-year-old woman was admitted to the hospital for jaundice since 14 days back. Besides generalized jaundice, the patient complained about vague abdominal pain and feeling of fullness. On physical examination, she showed tenderness on epigastric and right upper quadrant region. There was the presence of a palpable mass, about the size of an adult fist which was firm and tender to the touch. Initial laboratory studies revealed hemoglobin level of 9.2 g/dL (normal range, 14 to 18), white blood cell count of 6,000/mm3 (4,000 to 10,000) and a platelet count of 407,000/dL (140,000 to 400,000). The liver function tests showed a total serum bilirubin level of 4.7 mg/dL (0.1 to 1.2), an aspartate aminotransferase level of 205 IU/L (10 to 35), alanine aminotransferase level of 153 IU/L (0 to 40), alkaline phosphatase level of 1,532 IU/L (20 to 90), and a gamma glutamyl transpeptidase level of 260 IU/L (0 to 50). A computerized tomography scan (Fig. 1) revealed the presence of a huge irregular mass at the portocaval space measuring 14×8.5 cm, encircling the extrahepatic bile duct with mild dilatation of the intrahepatic bile duct. The mass infiltrated liver parenchyme and common hepatic artery was displaced to forward position by the mass. Also, portal vein and inferior vena cava were compressed. In the next step, we performed magnetic resonance cholangiopancreatography (MRCP) and found intra- and extra-hepatic bile duct dilatation with a filling defect at the hilar and common hepatic duct level (Fig. 2). Therefore, we carried out endoscopic retrograde cholangiopancreatography (ERCP) for the biliary decompression and to confirm the nature of the filling defect. At ERCP, we observed some fresh blood getting discharged from the papillary orifice when we injected contrast media into the bile duct (Fig. 3; inset). Cholangiography revealed mild dilatation of the bile duct with a filling defect, which moved downwards to the distal part of the bile duct when compared with the previous MRCP finding (Fig. 3). Through the endoscopic sphincterotomy and sweeping of the bile duct by balloon catheter, we ascertained that the filling defect was blood clots, which might be caused by direct tumor invasion of the bile duct. Subsequently, we inserted a biliary stent up to the hilar level for considering the progression of biliary obstruction due to presence of the mass. After the procedure, there was an improvement in the patient's general condition and there was also a decrease in the severity of the jaundice. For pathological confirmation, we carried out ultrasonography-guided biopsy on the mass. Pathologically, a poorly differentiated synovial sarcoma was diagnosed, which was immunoreactive for CD99 but negative for S-100, desmin, and smooth muscle actin (Fig. 4). After the confirmative diagnosis was carried out, we planned to perform chemoradiotherapy on the patient. But the patient refused any further treatment and was discharged from the hospital. Two weeks after getting discharged from the hospital, the patient returned for follow-up. She was in good condition except for the presence of abdominal fullness. The serum total bilirubin was 0.9 mg/dL, and there was a great improvement on other liver function tests. Nevertheless, 2 months later, the patient expired due to aggravation of the tumor.
 | Fig. 1(A) Axial image of abdomen computed tomography scan revealing the presence of a huge retroperitoneal mass (14×8.5 cm) with direct liver invasion (arrowheads) and compressed inferior vena cava (arrow). (B) Coronal image also reveals encircling of the extrahepatic bile duct by the tumor (arrows).
|
 | Fig. 2Magnetic resonance cholangiopancreatography shows the presence of a filling defect (arrow) at the hilar and common hepatic duct level of the bile duct.
|
 | Fig. 3Endoscopic retrograde cholangiopancreatography shows a tubular filling defect (arrow); we could verify that the filling defect was movable during the intrabiliary injection of the contrast media. Some fresh blood was discharged from the papillary orifice when contrast media was injected into the bile duct (arrow in the inset).
|
Go to :
DISCUSSION
Retroperitoneal synovial sarcoma usually appears as a nonspecific soft tissue mass that does not have specific imaging features and distinct clinical presentation for differentiation from other mesenchymal tumors. It usually has vague and nonspecific symptoms like abdominal pain, discomfort and tenderness with related pressure on adjacent structures.3,5 Therefore, most of the reported cases of retroperitoneal synovial sarcoma, up to now, have focused on its rarity, radiologic characteristics, pathological confirmative process, and their results. Recent studies have been focused on radiographic studies including computed tomography and magnetic resonance imaging, which can allow proper identification of the primary anatomic location of the tumor; they can also help in differentiating it from a tumor originating from retroperitoneal structure.6-8 However, these studies provide only suggestion about preoperative diagnosis of synovial sarcoma. Eventually, most of the retroperitoneal synovial sarcomas are diagnosed on the basis of pathological characteristics of the specimen obtained by needle or surgical resection.5 The present case also shows similar radiologic findings and diagnostic processes to the previously reported cases. Initially, we suspected the lesion to be a kind of sarcoma or lymphoma or other retroperitoneal tumors. The retroperitoneal synovial sarcoma could be diagnosed only after confirming the pathological findings of the needle biopsied specimen. However, our patient had unique and distinct clinical presentation with obstructive jaundice. With ERCP, the cause of obstructive jaundice was revealed to be the presence of intrabiliary blood clots with bile duct dilatation, which might be caused by bile duct injury from a tumor's invasion. Also, bile duct compression due to the presence of a bulk tumor might have also affected the presentation. After removal of the intrabiliary blood clots and biliary stenting, improvement in the severity of obstructive jaundice was observed. Unfortunately, the patient refused further treatment and finally died due to progression of the disease.
Go to :
 XML Download
XML Download