

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Postpolypectomy bleeding is the most common complication of colonoscoipc polypectomy, accounting for 0.3% to 6.1% of polypectomy.1,2 Bleeding can occur immediately following polypectomy or be delayed up to 30 days. The risk is related to the type and size of polyp, the technique of polypectomy, and the coagulation status of the patient. In most of cases, postpolypectomy bleeding can be controlled endoscopically.3,4 Therefore endoscopists should be aware of various techniques of colonoscopic hemostasis.
MANAGEMENT OF IMMEDIATE BLEEDING
Immediate bleeding has been reported in 1.5% to 2.8% following polypectomy.5 The risk increases when blended current is used and when cold snaring (pulling the snare without the use of cautery) is performed. Age of ≥65 years, cardiovascular or chronic renal disease, use of anticoagulants, polyp size greater than 1 cm, polyp morphology, poor bowel preparation, cutting mode of electrosurgical current, and inadvertent cutting of a polyp before current application are noted as independent risk factors for immediate bleeding.6 Most immediate bleeding can be controlled with various endoscopic techniques. The technique for hemostasis depends upon the severity of bleeding, the type of polyp, and individual preference. A combination of hemostasis techniques is frequently performed.7
Application of pressure
Especially for pedunculated polyps, immediate bleeding after polypectomy can easily be stopped by regrasping the pedicle with a snare and holding pressure on the pedicle to stop blood flow. After complete hemostasis of active bleeding, further techniques of bipolar cautery, injection, or endoclips can be applied.
Injection with epinephrine
A 1:10,000 dilution of epinephrine is commonly used, which is simply injected to the bleeding lesion. Epinephrine injection is frequently combined with other hemostatic techniques.
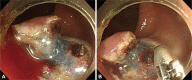
Cautery
Cautery is an effective method to treat a bleeding site (Fig. 1). It is done with thermal probes, bipolar cautery, or the tip of a polypectomy snare. Because the colon wall is very thin, the current should be decreased by approximately 50% relative to that used in the upper gastrointestinal tract. For heat probe, 15 J is safe and 10 to 15 W for bipolar cautery. When applying with thermal probes or bipolar cautery, endoscopists should not press the devices to the lesion, which increase the risk of perforation.
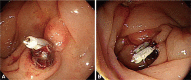
Hemoclips
Hemoclips is a safe and effective method to treat immediate bleeding. Sometimes it is difficult to approach a lesion with clips because of the location (Fig. 2). In these cases, cap device help to apply clips successfully. Previous study reported that 2.9±2 clips were required to achieve complete hemostasis.
MANAGEMENT OF DELAYED BLEEDING
Delayed bleeding occurs in up to 2% of patients receiving polypectomy.7 Delayed bleedings develops on average 5 to 7 days after polypectomy, but it can occur up to 30 days later. Polyp size is related to the risk of delayed bleeding from 1% for polyps less than 10 mm to 6.5% for those over 20 mm.8,9 Old age, hypertension, large sessile polyps, polyps at right colon, and polypectomy with pure coagulation are known as the risk factors for delayed bleeding. Non-steroidal anti-inflammatory drugs or aspirin use do not increase the risk of delayed bleeding.
Most delayed postpolypectomy bleeding can be managed successfully with colonoscopic techniques (Fig. 3). About half of patients who are admitted to hospital with hematochezia within 6 hours to 14 days after polypecotmy require blood transfusion. The timing of intervention depends on the amount and the rate of bleeding. Colonoscopy should be performed immediately in patients with active bleeding.10 Epinephrine injection, thermal therapy or hemoclips are usually performed alone or in combination.
CONCLUSIONS
Bleeding is the most common postpolypectomy complication frequently encountered by endoscopists. Most of bleeding can be effectively managed with endoscopic techniques. Therefore endoscopists should know and master various endoscopic techniques to treat postpolyectomy bleeding successfully.

 XML Download
XML Download