

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Kidney transplantation (KT) is the treatment of choice to improve patient quality of life and long-term survival in end-stage renal disease [1]. One significant obstacle to achieving a successful survival rate is increased malignancy-related mortality compared with the general population [123]. The risk of cancer in recipients is attributed mainly to chronic use of immunosuppressants and altered T-cell immunity [4]. Recently, transplants across immunologic barriers, including among patients with blood groups A and B and human leukocyte antigen (HLA) antibodies, have increased [5]. These immunologically high-risk transplant patients require desensitization treatment using plasmapheresis, rituximab (Genentech, Inc., San Francisco, CA, USA), and intravenous immunoglobulin (IVIG) and maintenance of a high concentration of a calcineurin inhibitor (CNI) [6]. Although intense immunosuppression provides a survival benefit for patients waiting for a compatible donor, side effects, including mortality from infectious complications, BK virus infection, and postoperative bleeding, are also increased [578].
Rituximab, an anti-CD20 monoclonal antibody that depletes peripheral blood B cells for 3–12 months, has been increasingly used for therapeutic purposes for pretransplant desensitization and rejection treatment after KT [9]. Host immune cells play a crucial role in antitumor mechanisms, and T cells have recently been applied to therapeutic advancements in cancer treatment such as chimeric antigen receptor-T cell therapies and checkpoint inhibitors [10]. B cells have also been found to play essential roles in suppressing tumor progression through humoral immunity and local immune reactions with tertiary lymphoid organs [3]. However, only a few studies with a small number of patients have evaluated the effect of rituximab on cancer development following KT [111213]. Furthermore, rituximab increases the risk of infectious complications, including viral, bacterial, and lethal fungal infections [1415]. Considering that immunosuppression increases the incidence of virus-related cancer, such as Kaposi sarcoma, cervical cancer, and hepatocellular carcinoma (HCC), and that East Asia is an endemic area of HBV infection, there is a need to evaluate the impact of rituximab treatment on cancer development [1617].
In this study, we reviewed the incidence of malignant disease in a large single-center cohort and evaluated the effect of rituximab on the cancer occurrence and mortality rate according to each type of cancer.
METHODS
Patients
This was a retrospective study using a database obtained by reviewing the medical records from Asan Medical Center (AMC) in Seoul, Korea. We included 5,000 consecutive recipients who underwent KT at AMC between January 1990 and January 2018. We divided the study cohort into era1 (1990–2007) and era2 (2008–2018) because our center started to perform HLA- and ABO-incompatible KT in 2008. The patients in era2 also were divided into non-rituximab (era2-rit–) and rituximab groups (era2-rit+) to evaluate the effect of rituximab. The era2-rit+ group included patients who received single-dose rituximab (200–500 mg) as a desensitization treatment 1–2 weeks before KT [5].
The Institutional Review Board of AMC approved this study (No. AMC 2021-0498) and waived informed consent due to the retrospective nature of this study using data from patients’ medical records. No organs/tissues were procured from any vulnerable populations, and all donors or next of kin provided written informed consent that was freely given. Organs/tissues were procured only at registered institutions with The Korean Network for Organ Sharing, which is a nationwide system of deceased donor detection and distribution.
Immunosuppression
When we started performing KT at our center in 1990, we used an immunosuppressive regimen consisting of cyclosporin, corticosteroids, and azathioprine without an induction drug. Since the mid-1990s, we have increased the usage of tacrolimus as a CNI, and more than 80% of recent transplant recipients have received tacrolimus. Azathioprine is no longer in use and has been replaced by mycophenolic acid. Patients have received basiliximab (Simulect, Novartis, East Hanover, NJ, USA) as an induction therapy since 1999. Recently, we have used rabbit antithymocyte globulin (Thymoglobulin, Genzyme, Cambridge, MA, USA) in highly sensitized recipients. In ABO-incompatible and crossmatch-positive KT, recipients receive a single dose of rituximab (200–500 mg) 2–3 weeks before transplantation and plasmapheresis with/without IVIG according to the desensitization protocol of our center [5].
Cancer screening
According to the National Cancer Screening Program (NCSP) in South Korea and our transplant program protocol, all transplant candidates undergo cancer screening [18]. We perform esophagogastroduodenoscopy (for patients aged ≥16 years), colonoscopy (for patients aged ≥40 years), and abdominal ultrasonography (USG). Non-contrast-enhanced abdominopelvic CT has replaced abdominal USG since November 2013. In addition, female patients undergo a Papanicolaou test with a gynecological examination and mammography, and male patients undergo measurement of PSA levels. After transplantation, we recommend that all recipients undergo cancer screening tests according to the NCSP guidelines. Patients with chronic HBV infection undergo abdominal USG and have α-FP levels evaluated every 6–12 months [19].
Statistical analysis
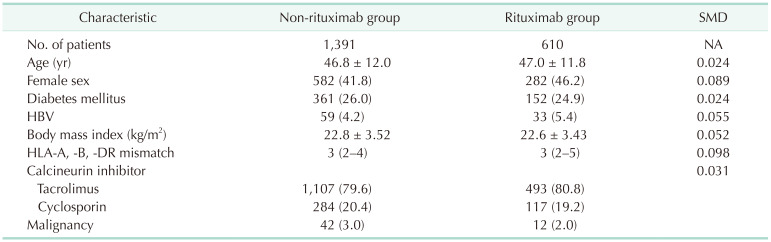
Categorical variables were assessed by the chi-square test and are presented as counts and percentages. Normally distributed continuous variables are shown as the mean ± standard deviation, and nonnormally distributed continuous variables are presented as medians and interquartile ranges (IQRs). Analysis of variance and the Kruskal-Wallis test were used to analyze continuous variables among the 3 groups, as appropriate. The survival rate was evaluated by Kaplan-Meier analysis and compared with the log-rank test. The risk factors for cancer and cancer-related mortality following KT were evaluated by univariate and multivariate Cox proportional hazards regression analysis. Recipients in the groups era2-rit– and era2-rit+ were selected by a maximum 3:1 match based on propensity scores. The variables for propensity matching included age, sex, body mass index (BMI), diabetes mellitus (DM), HBV infection, CNI, HLA mismatch, and living vs. deceased donor. A standardized difference of <0.1 was considered balanced. All statistical analyses were performed in IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA), and a P-value of 0.05 was considered a significant cutoff value.
RESULTS
Patient demographic and clinical characteristics
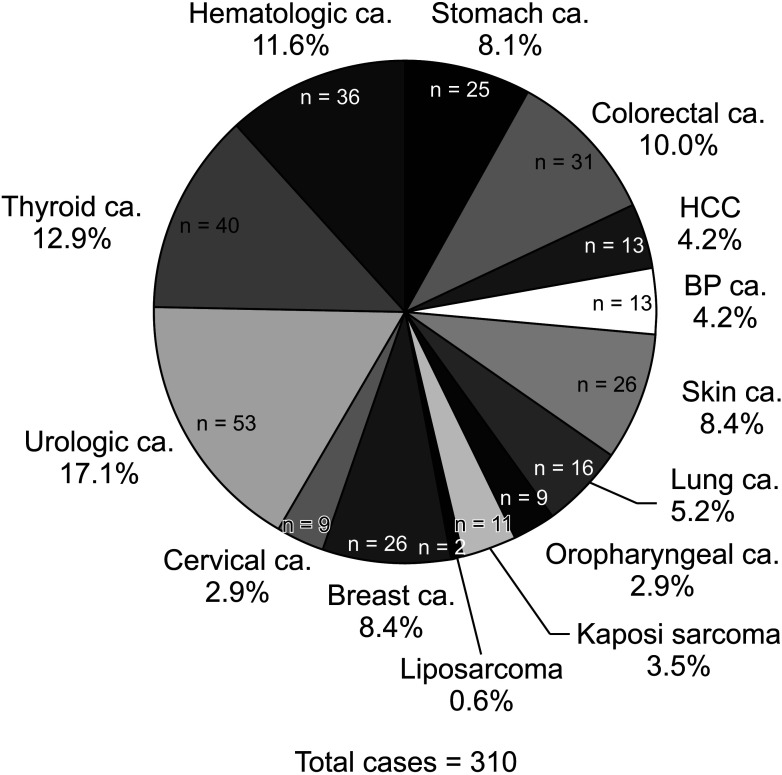
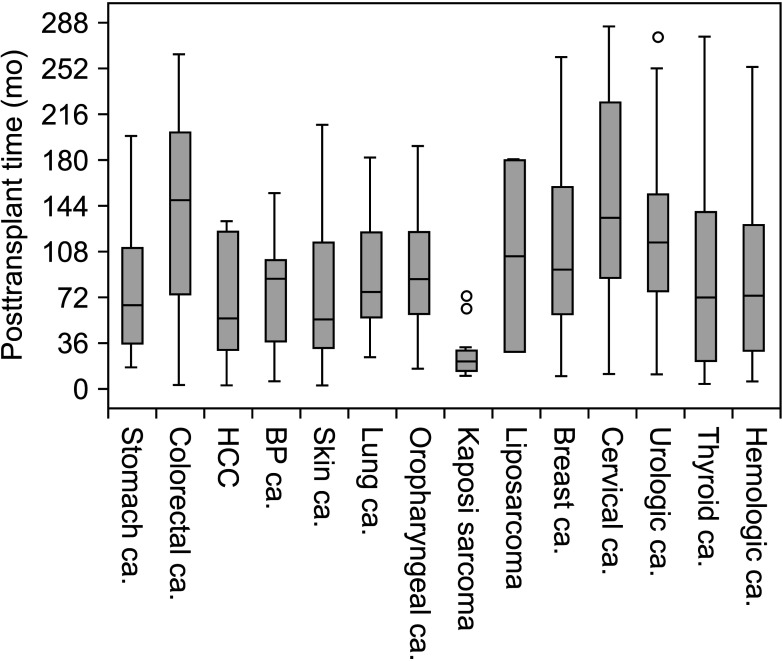
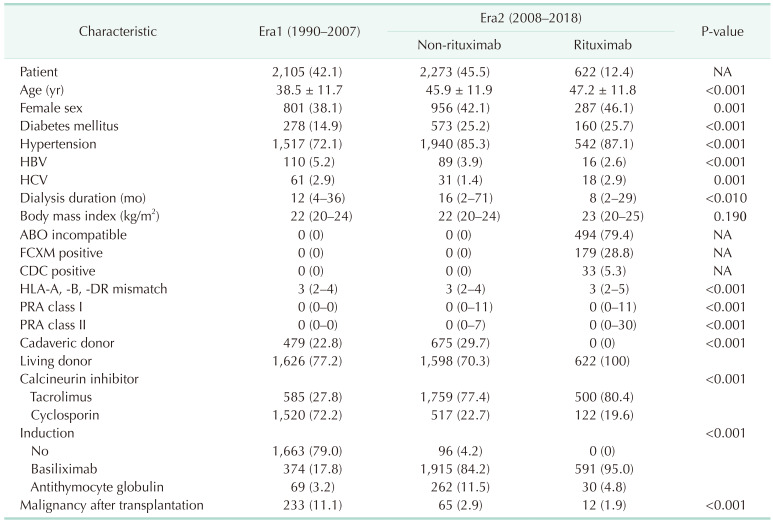
The 5,000 consecutive recipients who underwent KT at our center were divided into the era1 (n = 2,105, 42.1%), era2-rit– (n = 2,273, 45.5%), and era2-rit+ groups (n = 622, 12.4%). The baseline demographics of this study are demonstrated in Table 1. The era2-rit– and era2-rit+ groups had significantly higher proportions of older patients (P < 0.001), female patients (P = 0.001), patients with DM (P < 0.001), and patients with hypertension (P < 0.001) than the era1 group. More patients in the era1 group than in the other 2 groups were HBV carriers (P < 0.001). More patients in the era2-rit– and era2-rit+ groups than in the era1 group used tacrolimus instead of cyclosporin (P < 0.001). There were 233 (11.1%), 65 (2.9%), and 12 cases (1.9%) of posttransplant malignancies in the era1, era2-rit–, and era2-rit+ groups, respectively, during a mean follow-up period of 212± 78, 83 ± 37, and 72 ± 31 months, respectively (P < 0.001). Urologic malignancy was the most frequently identified cancer (n = 53, 17.1%) after KT, followed by thyroid (n = 40, 12.9%), hematologic (n = 36, 11.6%), colorectal (n = 31, 10.0%), breast (n = 26, 8.4%), and stomach (n = 25, 8%) cancer (Fig. 1). The median (IQR) time from transplantation to cancer occurrence was 21 months (14–33 months) for Kaposi sarcoma, 54 months (32–116 months) for skin cancer, 56 months (20–126 months) for HCC, 66 months (35–115 months) for stomach cancer, 72 months (21–141 months) for thyroid cancer, 73 months (29–129 months) for hematologic cancer, 76 months (53–124 months) for lung cancer, 87 months (27–103 months) for biliary-pancreatic (BP) cancer, 94 months (58–160 months) for breast cancer, 115 months (73–157 months) for urologic cancer, and 148 months (73–204 months) for colorectal cancer (Fig. 2).
Risk factors for cancer-related mortality
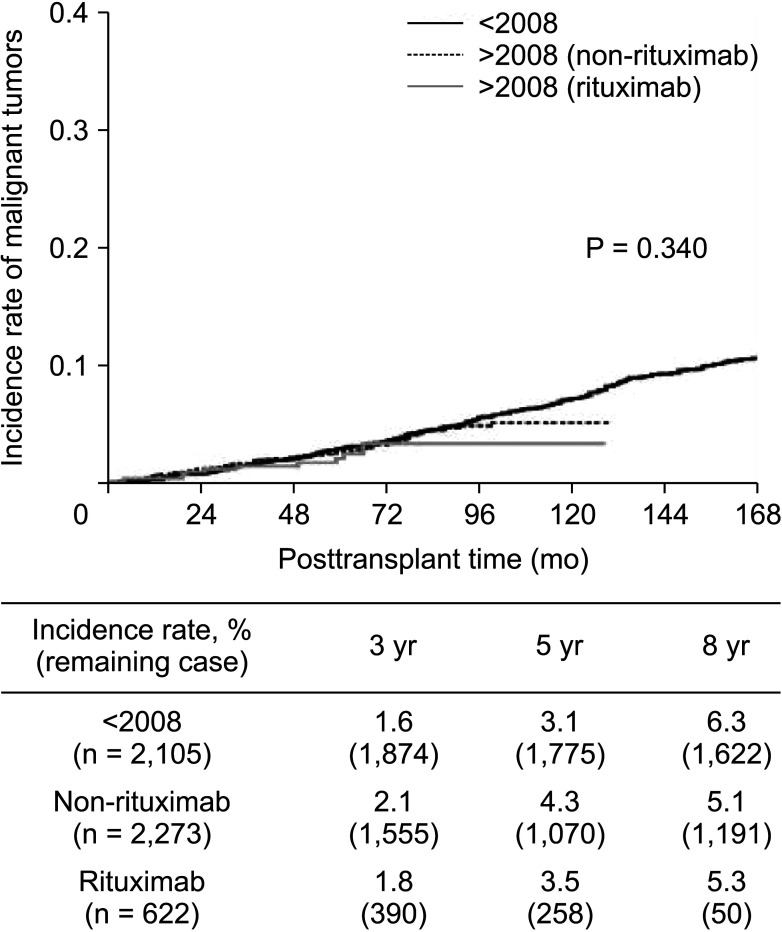
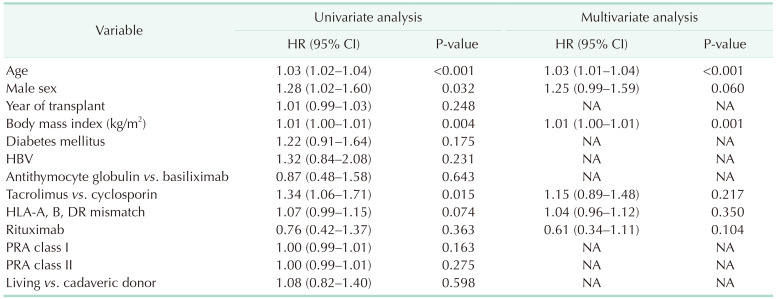
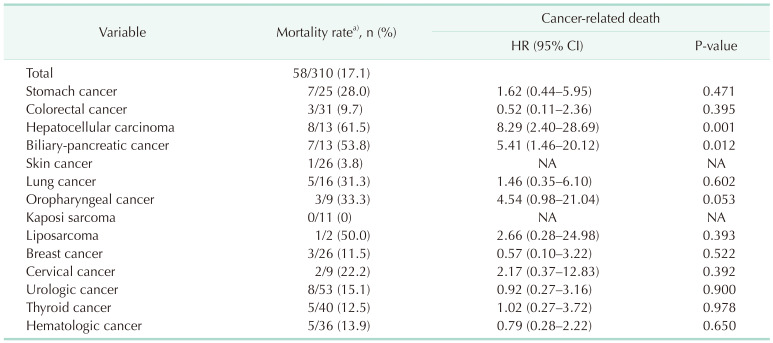
In the multivariate regression analysis, age (hazard ratio [HR], 1.03; 95% confidence interval [CI], 1.01–1.04; P < 0.001) and BMI (HR, 1.01; 95% CI, 1.00–1.01; P = 0.001) were significant risk factors for malignant disease after transplant. However, rituximab had no significant association (Table 2). The propensity match analysis showed that rituximab did not increase the risk of cancer following KT HCC (HR, 1.36; 95% CI, 0.72–2.57; P = 0.348) (Table 3). The overall cancer-related mortality rate was 17.1% (53 of 310). HCC (61.5%) had the highest mortality rate, followed by BP (53.8%), lung (31.3%), oropharyngeal (33.3%), and stomach cancer (28.0%). The relative risk of cancer-related death stratified by the type of malignancy was significantly high among patients with HCC (HR, 8.29; 95% CI, 2.40–28.69; P = 0.001), BP cancer (HR, 5.41; 95% CI, 1.46–20.12; P = 0.012), and oropharyngeal cancer (HR, 4.54; 95% CI, 0.98–21.04; P = 0.053) after adjusting for the following risk factors; age, BMI, sex, DM, and rituximab treatment (Table 4). The 5-year incidence rates of malignant tumors after KT were 3.1%, 4.3%, and 3.5% in the era1, era2-rit–, and era2-rit+ group, respectively. The overall incidence rate of cancer after transplantation among the 3 study groups showed no significant difference (P = 0.340) (Fig. 3).
Clinical characteristics and outcomes of hepatocellular carcinoma
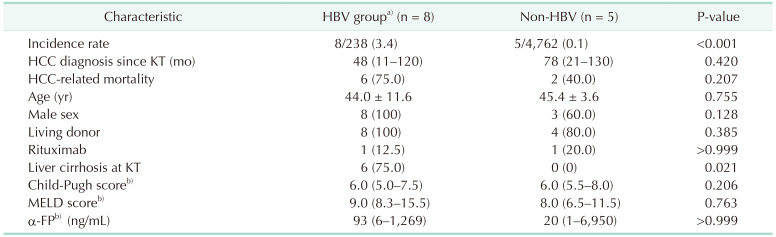
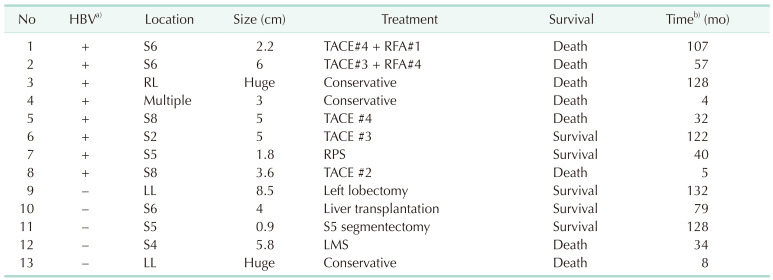
Out of the 5,000 recipients, there were 238 patients (4.8%) who were chronic HBV carriers, and 4,762 (95.2%) who were non-HBV-infected patients. There were 8 chronic HBV carriers (3.4%) and 5 (non-HBV carriers 0.1%) who developed HCC (P < 0.001). The HCC-related mortality was 6 out of 8 cases (75.0%) in the HBV group and 2 out of 5 cases (40.0%) in the non-HBV group (P = 0.210). Among both the HBV and non-HBV carriers who were transplant recipients, only 1 patient who developed HCC was treated with rituximab for pretransplant desensitization. Six patients among 8 patients (75.0%) with HCC in the HBV group showed liver cirrhosis at the time of KT. Otherwise, there were no significant differences between HBV and non-HBV carriers who developed HCC, including age, sex, Child-Pugh score, Model for End-Stage Liver Disease (MELD) score, and α-FP level (Table 5). The clinical course and outcomes of 13 patients who developed HCC are shown in Table 6. After adjusting for age, DM, BMI, sex, rituximab, CNI, HBV, and HCV, we found that HBV (HR, 25.2; 95% CI, 7.94–79.86; P < 0.010) was the only significant risk factor for the development of HCC in the multivariate regression analysis.
DISCUSSION
Our study revealed that rituximab did not affect the incidence of overall cancer development or that of each type of cancer. The malignancy-related mortality rate also showed no difference between the era2-rit– and era2-rit+ groups. The overall cancer incidence rate (310 cases, 6.2%) and mortality rate (58 cases, 1.2%) during 136 ± 87 months of the follow-up period were similar to those reported in recent studies [320]. However, our cohort had a relatively higher incidence and mortality rate of HCC than those in other studies performed in nonendemic area of HBV infection [320]. HCC was associated with the highest risk of cancer-related mortality among all cancer types that developed after transplantation in our study.
There has been little research on the risk of secondary malignancies due to rituximab treatment. Schrezenmeier et al. [13] reported that only 1 case of malignancy among 63 patients treated with rituximab. Bachelet et al. [11] also did not find an association between rituximab and an increased risk of posttransplant malignancy even though the recipients received antithymocyte globulin induction. These studies were conducted on a small number of patients to evaluate the effect of rituximab. By studying 622 patients who received rituximab, we evaluated the association between rituximab and cancer occurrence following transplantation more fully than recent studies. Although the follow-up period between the era1 and era2 groups was different, considering that the effects of rituximab usually do not exceed 12 months, our results were obtained with a sufficient observation period [9]. T-cell depletion with induction treatment and maintenance with tacrolimus rather than cyclosporin have been reported as risk factors for developing de novo tumors after transplantation [21]. Rituximab has been reported to increase the risk of secondary solid tumors in lymphoma treatment with high-dose chemotherapy [22]. However, B-cell depletion associated with single-dose rituximab does not seem to have enough of an impact on the development of cancer.
Rituximab increases complication rates from infectious diseases, including viral, bacterial, and fungal infections, mostly when a dosage greater than standard-dose rituximab (375 mg/m2) is used [523]. Recent studies have shown that viral infections such as infections with human herpesvirus type 9, Epstein Barr virus, human papillomavirus, HBV, and HCV increase the risk of malignant disease associated with their pathogenesis [24]. Therefore, in contrast to our study results, we assumed that rituximab could increase the rate of cancer development. One of the reasons we suspect that rituximab did not increase the cancer risk was that a low dose of less than 200 mg/m2 was used. We previously experienced lethal infectious complications when we used a desensitization protocol with 500 mg of rituximab [5]. After modifying the protocol to use 200 mg of rituximab, we significantly reduced the infectious complications and achieved a patient survival rate similar to that achieved with ABO- and HLA-compatible recipients [5]. Although 102 patients who received 500 mg of rituximab did not have increased cancer incidence or cancer-related mortality in our multivariate analysis, considering that 7 patients died due to early complications and only a small number of patients received 500 mg of rituximab, the modified desensitization protocol seemed to play a critical role in reducing infectious complications and related malignancies. In addition, recent research has shown that reduced-dose rituximab can prevent HBV reactivation after transplantation [25].
HBV infection is the primary cause of HCC, accounting for up to 75% of HCC cases [26]. Our study also showed that patients with HBV had a significantly higher rate of HCC after KT than those without HBV. The incidence rate of HCC (3.4%) in HBV-infected patients in our study was similar to the results of Kanaan et al. [17], showing outcomes of HBV- and HCV-associated HCC after KT. The incidence rate appears to be lower than that of the general population possibly because only patients with compensated liver cirrhosis underwent KT and recipients were thoroughly screened before and after transplantation. Although we did not find a relationship between HCC incidence and rituximab, the risk of cancer-related mortality was the highest in HCC among all kinds of cancer. All 8 patients who developed HCC among HBV-infected patients underwent pre- and postoperative screening examinations as scheduled. However, 6 patients died due to HCC aggravation, and 2 patients among these 6 patients developed HCC within 6 months after transplantation. Therefore, the current guidelines for HCC for patients with HBV infection may need to be modified in terms of the diagnostic modalities and testing period. Six out of 8 patients who developed HCC had liver cirrhosis identified on preoperative nonenhanced CT or USG. Currently, USG is the backbone of HCC surveillance [19]. Nevertheless, a recent meta-analysis reported that the sensitivity of USG is low for identifying early-stage HCC in patients with liver cirrhosis [27]. CT and MRI have been suggested to be more accurate diagnostic tools [272829]. In a randomized trial, Pocha et al. [29] reported that CT showed no significant differences in sensitivity and sensitivity from USG for detecting any stage of HCC. Kim et al. [28] demonstrated that MRI with liver-specific contrast had a higher HCC detection rate than USG in patients with cirrhosis. The surveillance interval is also an important factor in detecting early HCC in patients with cirrhosis. There was a report that a surveillance interval with USG within 6 months improved sensitivity for diagnosing early HCC compared with annual surveillance [30]. Additional enhanced CT or MRI scans as preoperative screening tools may prevent aggravation of hidden HCC after transplantation in patients with HBV and cirrhosis. We also recommend that recipients with liver cirrhosis undergo surveillance tests at least every 6 months.
Our study has limitations due to its retrospective nature and because it was conducted in a single center for over 30 years. The immunosuppressive protocols, antiviral therapy for HBV, and diagnostic techniques and treatment options for malignant diseases have been changed. To overcome confounders associated with time variation, we performed a Cox proportional hazards regression analysis and divided the study groups according to the era. We did not compare cancer risk and cancer-related mortality in our cohort with those in the general population. We focused on evaluating the risks associated with rituximab treatment in KT recipients. In addition, as most of the recipients enrolled in this study were of Asian descent, our results may not be applicable to patients of other races. However, this study yielded a novel finding about HBV-carrying recipients by including a relatively large number of patients compared with nonendemic areas. Finally, cancer that occurred among patients who were not followed up in our center may have led to an underestimation of the incidence of malignant tumors. However, our study was able to utilize more accurate information as a single institutional study compared to a large-scale cohort study.
Our results suggest that single-dose rituximab for desensitization may not increase the risk of malignant disease or cancer-related mortality in recipients undergoing KT. HCC was associated with the highest risk of cancer-related mortality in our study cohort. To reduce the HCC-related mortality, enhanced CT or MRI can be helpful diagnostic modalities to enhance the sensitivity and specificity for early detection of HCC in patients with liver cirrhosis. We also recommend that the surveillance interval not exceed 6 months.
 XML Download
XML Download