1. Lee MS. Guideline for management of ruptured aneurysm: preliminary report. Neurointervention. 2007; 2:36–42.
2. Kim KH. Guideline for management of unruptured intracranial aneurysms: preliminary report. Neurointervention. 2007; 2:43–49.
3. Shin SH, Kwon SC, Suh DC. Recent update of guidelines for neurointerventional procedures. Neurointervention. 2013; 8:68–72. PMID:
24024069.

4. Bederson JB, Connolly ES Jr, Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the stroke council, American Heart Association. Stroke. 2009; 40:994–1025. PMID:
19164800.
5. Connolly ES Jr, Rabinstein AA, Carhuanpoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Assocation. Stroke. 2012; 43:1711–1737. PMID:
22556195.
6. Mayberg MR, Batjer HH, Dacey R, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 1994; 25:2315–2328. PMID:
7974568.
7. Cortnum S, Sorensen P, Jorgensen J. Determining the sensitivity of computed tomography scanning in early detection of subarachnoid hemorrhage. Neurosurgery. 2010; 66:900–902. PMID:
20404693.
8. Fiebach JB, Schellinger PD, Geletneky K, et al. MRI in acute subarachnoid haemorrhage; findings with a standardised stroke protocol. Neuroradiology. 2004; 46:44–48. PMID:
14655034.
9. Kidwell CS, Wintermark M. Imaging of intracranial haemorrhage. Lancet Neurol. 2008; 7:256–267. PMID:
18275927.
10. Shimoda M, Hoshikawa K, Shiramizu H, Oda S, Matsumae M. Problems with diagnosis by fluid-attenuated inversion recovery magnetic resonance imaging in patients with acute aneurysmal subarachnoid hemorrhage. Neurol Med Chir (Tokyo). 2010; 50:530–537. PMID:
20671377.
11. Steiner T, Juvela S, Unterberg A, Jung C, Forsting M, Rinkel G. European Stroke Organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrahge. Cerebrovasc Dis. 2013; 35:93–112. PMID:
23406828.
12. Donmez H, Serifov E, Kahriman G, Mavili E, Durak AC, Menku A. Comparison of 16-row multislice CT angiography with conventional angiography for detection and evaluation of intracranial aneurysms. Eur J Radiol. 2011; 80:455–461. PMID:
20729022.
13. Jayaraman MV, Mayo-Smith WW, Tung GA, et al. Detection of intracranial aneurysms: multi-detector row CT angiography compared with DSA. Radiology. 2004; 230:510–518. PMID:
14699177.
14. Kadri S, Brunel H, Bourbotte G, Delort P, Lust S, Bonafe A. Can multislice helical computed tomography replace conventional angiography in the diagnosis of non traumatic subarachnoid hemorrhage? J Neuroradiol. 2006; 33:45–50. PMID:
16528205.
15. McKinney AM, Palmer CS, Truwit CL, Karagulle A, Teksam M. Detection of aneurysms by 64-section multidetector CT angiography in patients acutely suspected of having an intracranial aneurysm and comparison with digital subtraction and 3D rotational angiography. AJNR Am J Neuroradiol. 2008; 29:594–602. PMID:
18065510.
16. Agid R, Andersson T, Almqvist H, et al. Negative CT angiography findings in patients with spontaneous subarachnoid hemorrhage: When is digital subtraction angiography still needed? AJNR Am J Neuroradiol. 2010; 31:696–705. PMID:
19942709.
17. Brinjikji W, Kallmes DF, White JB, Lanzino G, Morris JM, Cloft HJ. Inter- and intraobserver agreement in CT characterization of nonaneurysmal perimesencephalic subarachnoid hemorrhage. AJNR Am J Neuroradiol. 2010; 31:1103–1105. PMID:
20075084.
18. Romijn M, Gratama van, van Walderveen MA, et al. Diagnostic accuracy of CT angiography with matched mask bone elimination for detection of intracranial aneurysms: Comparison with digital subtraction angiography and 3D rotational angiography. AJNR Am J Neuroradiol. 2008; 29:134–139. PMID:
17928381.
19. Zhang LJ, Wu SY, Niu JB, et al. Dual-energy CT angiography in the evaluation of intracranial aneurysms: Image quality, radiation dose, and comparison with 3D rotational digital subtraction angiography. AJR Am J Roentgenol. 2010; 194:23–30. PMID:
20028901.
20. White PM, Teasdale EM, Wardlaw JM, Easton V. Intracranial aneurysms: CT angiography and MR angiography for detection prospective blinded comparison in a large patient cohort. Radiology. 2001; 219:739–749. PMID:
11376263.
21. Agid R, Lee SK, Willinsky RA, Farb RI, terBrugge KG. Acute subarachnoid hemorrhage: Using 64-slice multidetector CT angiography to "triage" patients' treatment. Neuroradiology. 2006; 48:787–794. PMID:
17009025.
22. Ishihara H, Kato S, Akimura T, Suehiro E, Oku T, Suzuki M. Angiogram-negative subarachnoid hemorrhage in the era of three dimensional rotational angiography. J Clin Neurosci. 2007; 14:252–255. PMID:
17258133.
23. van Rooij WJ, Peluso JP, Sluzewski M, Beute GN. Additional value of 3D rotational angiography in angiographically negative aneurysmal subarachnoid hemorrhage: How negative is negative? AJNR Am J Neuroradiol. 2008; 29:962–966. PMID:
18258701.
24. Doelken M, Struffert T, Richter G, et al. Flat-panel detector volumetric CT for visualization of subarachnoid hemorrhage and ventricles: Preliminary results compared to conventional CT. Neuroradiology. 2008; 50:517–523. PMID:
18330518.
25. Murayama Y, Nien YL, Duckwiler G, Gobin YP, Jahan R, Frazee J, et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years' experience. J Neurosurg. 2003; 98:959–966. PMID:
12744354.
26. Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005; 366:809–817. PMID:
16139655.
27. Bakker NA, Metzemaekers JD, Groen RJ, Mooij JJ, Van Dijk JM. International subarachnoid aneurysm trial 2009: endovascular coiling of ruptured intracranial aneurysms has no significant advantage over neurosurgical clipping. Neurosurgery. 2010; 66:961–962. PMID:
20404700.
28. Risselada R, Lingsma HF, Bauer-Mehren A, et al. Prediction of 60 day case-fatality after aneurysmal subarachnoid haemorrhage: Results from the International Subarachnoid Aneurysm Trial (ISAT). Eur J Epidemiol. 2010; 25:261–266. PMID:
20155439.
29. Ioannidis I, Lalloo S, Corkill R, Kuker W, Byrne JV. Endovascular treatment of very small intracranial aneurysms. J Neurosurg. 2010; 112:551–556. PMID:
19715422.
30. Graves EJ. National hospital discharge survey. Vital Health Stat 13. 1992; 1–62.
31. Broderick JP, Brott TG, Duldner JE, Tomsick T, Leach A. Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke. 1994; 25:1342–1347. PMID:
8023347.
32. Raaymakers TW, Rinkel GJ, Ramos LM. Initial and follow-up screening for aneurysms in families with familial subarachnoid hemorrhage. Neurology. 1998; 51:1125–1130. PMID:
9781541.
33. Ronkainen A, Miettinen H, Karkola K, et al. Risk of harboring an unruptured intracranial aneurysm. Stroke. 1998; 29:359–362. PMID:
9472874.
34. Jakubowski J, Kendall B. Coincidental aneurysms with tumours of pituitary origin. J Neurol Neurosurg Psychiatry. 1978; 41:972–979. PMID:
712374.
35. Preul MC, Cendes F, Just N, Mohr G. Intracranial aneurysms and sickle cell anemia: multiplicity and propensity for the vertebrobasilar territory. Neurosurgery. 1998; 42:971–977. PMID:
9588540.
36. Asai A, Matsutani M, Kohno T, Fujimaki T, Takakura K. Multiple saccular cerebral aneurysms associated with systemic lupus erythematosus--case report. Neurol Med Chir (Tokyo). 1989; 29:245–247. PMID:
2477731.
37. Xu HW, Yu SQ, Mei CL, Li MH. Screening for intracranial aneurysm in 355 patients with autosomal-dominant polycystic kidney disease. Stroke. 2011; 42:204–206. PMID:
21164130.
38. Huston J 3rd, Torres VE, Sulivan PP, Offord KP, Wiebers DO. Value of magnetic resonance angiography for the detection of intracranial aneurysms in autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1993; 3:1871–1877. PMID:
8338918.
39. Mariani L, Bianchetti MG, Schroth G, Seiler RW. Cerebral aneurysms in patients with autosomal dominant polycystic kidney disease--to screen, to clip, to coil? Nephrol Dial Transplant. 1999; 14:2319–2322. PMID:
10528652.
40. Schievink WI. Marfan syndrome and intracranial aneurysms. Stroke. 1999; 30:2767–2768. PMID:
10583939.
41. Schievink WI, Riedinger M, Maya MM. Frequency of incidental intracranial aneurysms in neurofibromatosis type 1. Am J Med Genet A. 2005; 134A:45–48. PMID:
15690406.
42. Adachi K, Kudo M, Chen MN, Nakazawa S, Wakabayashi I. Cerebral aneurysm associated with multiple endocrine neoplasia, type 1--case report. Neurol Med Chir (Tokyo). 1993; 33:309–331. PMID:
7687038.
43. Munyer TP, Margulis AR. Pseudoxanthoma elasticum with internal carotid artery aneurysm. AJR Am J Roentgenol. 1981; 136:1023–1024. PMID:
6784505.
44. Defillo A, Nussbaum ES. Intracranial aneurysm formation in siblings with pseudoxanthoma elasticum: case report. J Neurosurg Sci. 2010; 54:105–107. PMID:
21423077.
45. Maher CO, Piepgras DG, Brown RD Jr, Friedman JA, Pollock BE. Cerebrovascular manifestations in 321 cases of hereditary hemorrhagic telangiectasia. Stroke. 2001; 32:877–882. PMID:
11283386.
46. de Paepe A, van Landegem W, de Keyser F, de Reuck J. Association of multiple intracranial aneurysms and collagen type III deficiency. Clin Neurol Neurosurg. 1988; 90:53–56. PMID:
3359734.
47. David CA, Vishteh AG, Spetzler RF, Lemole M, Lawton MT, Partovi S. Late angiographic follow-up review of surgically treated aneurysms. J Neurosurg. 1999; 91:396–401. PMID:
10470813.
48. Wermer MJ, Koffijberg H, van der Schaaf IC. Effectiveness and costs of screening for aneurysms every 5 years after subarachnoid hemorrhage. Neurology. 2008; 70:2053–2062. PMID:
18420481.
49. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation. 2000; 102:2300–2308. PMID:
11056108.
50. Raaymakers TW. Aneurysms in relatives of patients with subarachnoid hemorrhage: frequency and risk factors. MARS Study Group. Magnetic Resonance Angiography in Relatives of patients with Subarachnoid hemorrhage. Neurology. 1999; 53:982–988. PMID:
10496256.
51. Kuehn BM. FDA warning: CT scans exceeded proper doses. JAMA. 2010; 303:124. PMID:
20068201.
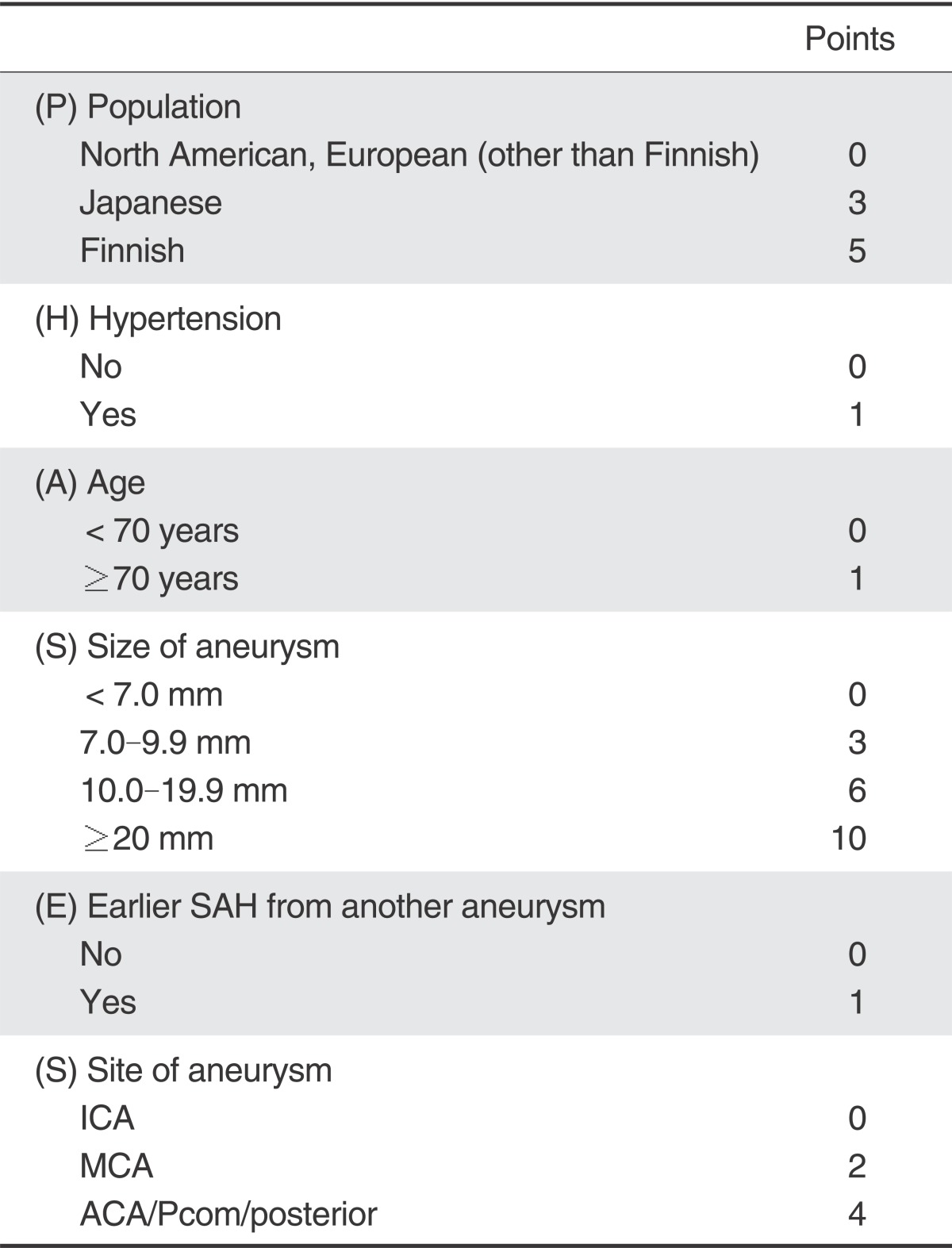
52. Greving JP, Wermer MJ, Brown RD Jr, et al. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol. 2014; 13:59–66. PMID:
24290159.
53. Wiebers DO, Whisnant JP, Huston J 3rd, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003; 362:103–110. PMID:
12867109.
54. Sonobe M, Yamazaki T, Yonekura M, Kikuchi H. Small unruptured intracranial aneurysm verification study: SUAVe study, Japan. Stroke. 2010; 41:1969–1977. PMID:
20671254.
55. UCAS Japan Investigators. Morita A, Kirino T, Hashi K, et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med. 2012; 366:2474–2482. PMID:
22738097.
56. Hasan DM, Mahaney KB, Brown RD Jr, et al. Aspirin as a promising agent for decreasing incidence of cerebral aneurysm rupture. Stroke. 2011; 42:3156–3162. PMID:
21980208.
57. Wiebers DO. Unruptured intracranial aneurysms: natural history and clinical management. Update on the international study of unruptured intracranial aneurysms. Neuroimaging Clin N Am. 2006; 16:383–390. PMID:
16935706.
58. Morita A, Fujiwara S, Hashi K, Ohtsu H, Kirino T. Risk of rupture associated with intact cerebral aneurysms in the Japanese population: a systematic review of the literature from Japan. J Neurosurg. 2005; 102:601–606. PMID:
15871500.
59. Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke. 1998; 29:251–256. PMID:
9445359.
60. Kim JE, Lim DJ, Hong CK, Joo SP, Yoon SM, Kim BT. Treatment of unruptured intracranial aneurysms in South Korea in 2006 : a nationwide multicenter survey from the korean society of cerebrovascular surgery. J Korean Neurosurg Soc. 2010; 47:112–118. PMID:
20224709.
61. Moroi J, Hadeishi H, Suzuki A, Yasui N. Morbidity and mortality from surgical treatment of unruptured cerebral aneurysms at Research Institute for Brain and Blood Vessels-Akita. Neurosurgery. 2005; 56:224–231. PMID:
15670370.
62. Krisht AF, Gomez J, Partington S. Outcome of surgical clipping of unruptured aneurysms as it compares with a 10-year nonclipping survival period. Neurosurgery. 2006; 58:207–216. PMID:
16462473.
63. Lanterna LA, Tredici G, Dimitrov BD, Biroli F. Treatment of unruptured cerebral aneurysms by embolization with guglielmi detachable coils: case-fatality, morbidity, and effectiveness in preventing bleeding--a systematic review of the literature. Neurosurgery. 2004; 55:767–775. PMID:
15458585.
64. van Rooij WJ, Sluzewski M. Procedural morbidity and mortality of elective coil treatment of unruptured intracranial aneurysms. AJNR Am J Neuroradiol. 2006; 27:1678–1680. PMID:
16971613.
65. Higashida RT, Lahue BJ, Torbey MT, Hopkins LN, Leip E, Hanley DF. Treatment of unruptured intracranial aneurysms: a nationwide assessment of effectiveness. AJNR Am J Neuroradiol. 2007; 28:146–151. PMID:
17213445.
66. Moret J, Cognard C, Weill A, Castaings L, Rey A. Reconstruction technic in the treatment of wide-neck intracranial aneurysms. Long-term angiographic and clinical results. Apropos of 56 cases. J Neuroradiol. 1997; 24:30–44. PMID:
9303942.
67. D'Urso PI, Lanzino G, Cloft HJ, Kallmes DF. Flow diversion for intracranial aneurysms: a review. Stroke. 2011; 42:2363–2368. PMID:
21737793.


 PDF
PDF ePub
ePub Citation
Citation Print
Print


 XML Download
XML Download