

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dilated medullary veins and a prominent draining venous structure constitute a typical developmental venous anomaly (DVA) and it is considered as a benign entity because it barely is associated with any neurological presentations [1]. DVAs associated with arteriovenous shunt causing intracerebral hemorrhages (ICHs) were reported but they are very rare [2-4], and atypical parenchymal type of arteriovenous malformation (AVM) mimicking DVAs were categorized only recently [5]. These clearly suggest DVAs are not a homogenous group of clinical benignancy, rather a diverse vascular anomaly with various findings.
Thrombosis of a DVA is extremely rare, 21 DVAs with thrombosis in the collecting veins were reported in the previous literatures [1, 6]. Those cases included 18 supratentorial and three infratentorial cases and showed image findings at initial diagnostic brain imaging mostly. But, serial changes during resolution and recanalization of the thrombosed DVA had not been documented with multimodal image findings.
We present a case of symptomatic DVA presented with hemorrhagic cerebral venous infarction in which repeated multimodal imaging clearly showed temporal changes of the thrombosed collecting vein and the affected brain.
CASE REPORT
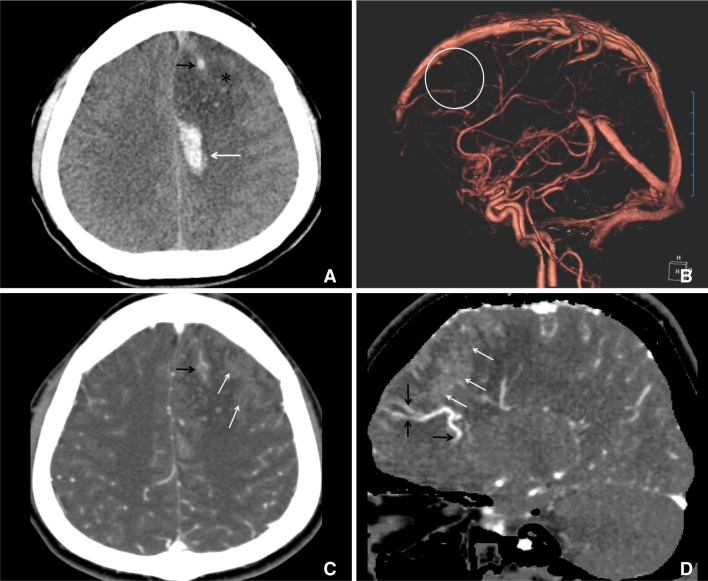
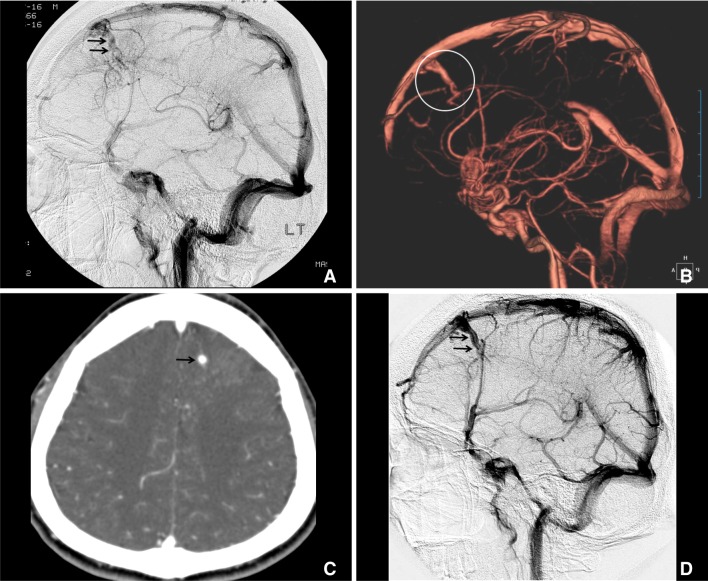
A 31-year-old male presented with loss of consciousness of abrupt onset after several days of headache. Initial pre-contrast CT showed swollen hypodense area, ICHs and linear hyperdensity in the left frontal lobe (Fig. 1A). CT angiography with 3-dimensional post processing revealed dilated medullary veins with caput medusa appearance, but no venous drainage from the left frontal DVA) (Fig. 1B-D). Multiplanar source images of CT angiography demonstrated the filling defect in the anterior superior sagittal venous sinus and suggested the thrombosis in the draining vein (Fig. 1C). On follow-up CT angiograms ten days (not shown in this report) and two months later (Fig. 2B, C), thrombosed draining vein was progressively recanalized and detected were findings of venous infarction with multifocal parenchymal hemorrhages in the left frontal lobe. Repeated digital subtraction angiography two years after the initial clinical presentation (Fig. 2D) clearly showed the presence of resolving venous thrombosis at a month (Fig. 2A).
No underlying cause such as connective tissue disease, coagulopathy, history of steroid administration, dehydration and so on was identified for the spontaneous thrombosis in the venous drainage from DVA.
The patient was treated conservatively, became conscious five days later and eventually recovered without localized neurological deficit. He developed generalized seizure, but had been under control with anti-epileptic medications.
DISCUSSION
In this case, interpretation of CT and CT angiography findings at the time of initial clinical presentation was complicated because spontaneous ICHs abruptly occurred in a young, healthy male and there was no underlying vascular pathology found such as AVM in the left frontal lobe or dural AVM and the hemorrhages appeared not to be related to neoplasms. Hypodense area in the left lobe involved both cortical gray matter and white matter as in the case of cerebral infarction, did not coincide with the territory of left anterior cerebral artery. Curvilinear hyperdensity coursed from the left frontal parenchyma to the midline anteriorly. Source images from CT angiography showed multiple dilated linear enhancements with parenchymal staining in the left frontal lobe. Possible venous infarction due to thrombosis in the venous drainage was suspected but DVA with thrombosis was not included in the initial differential diagnosis because venous collector was not recognizable. Early correct recognition of thrombosed typical DVA as the underlying cause for the ICH and venous infarction of sudden onset could lead to the proper anticoagulation treatment.
Cases of spontaneous ICH related to DVA were reported and associated with either high flow arteriovenous shunts or cavernous venous malformations [1-4]. However, very small number of typical DVAs were reported, which presented ICH as the initial manifestation [7, 8]. Seki et al. [9] analyzed previously reported 13 cases and their one case of typical DVA complicated by thrombosis of the draining vein. Among those 14 cases, they include one case of venous infarction without ICH by mistake, thus four had ICHs. eight cases of venous infarction including their own two were analyzed by Masson et al [10]. A case of childhood DVA complicated by spontaneous thrombosis was reported elsewhere [11] and should be included in the list of venous infarction. Among those nine, two were categorized as "hemorrhagic" and we reviewed the case reports. Authors of the two case reports related ICHs to thrombosis in the draining veins, and their case figures did not show venous infarction initially [8, 12].
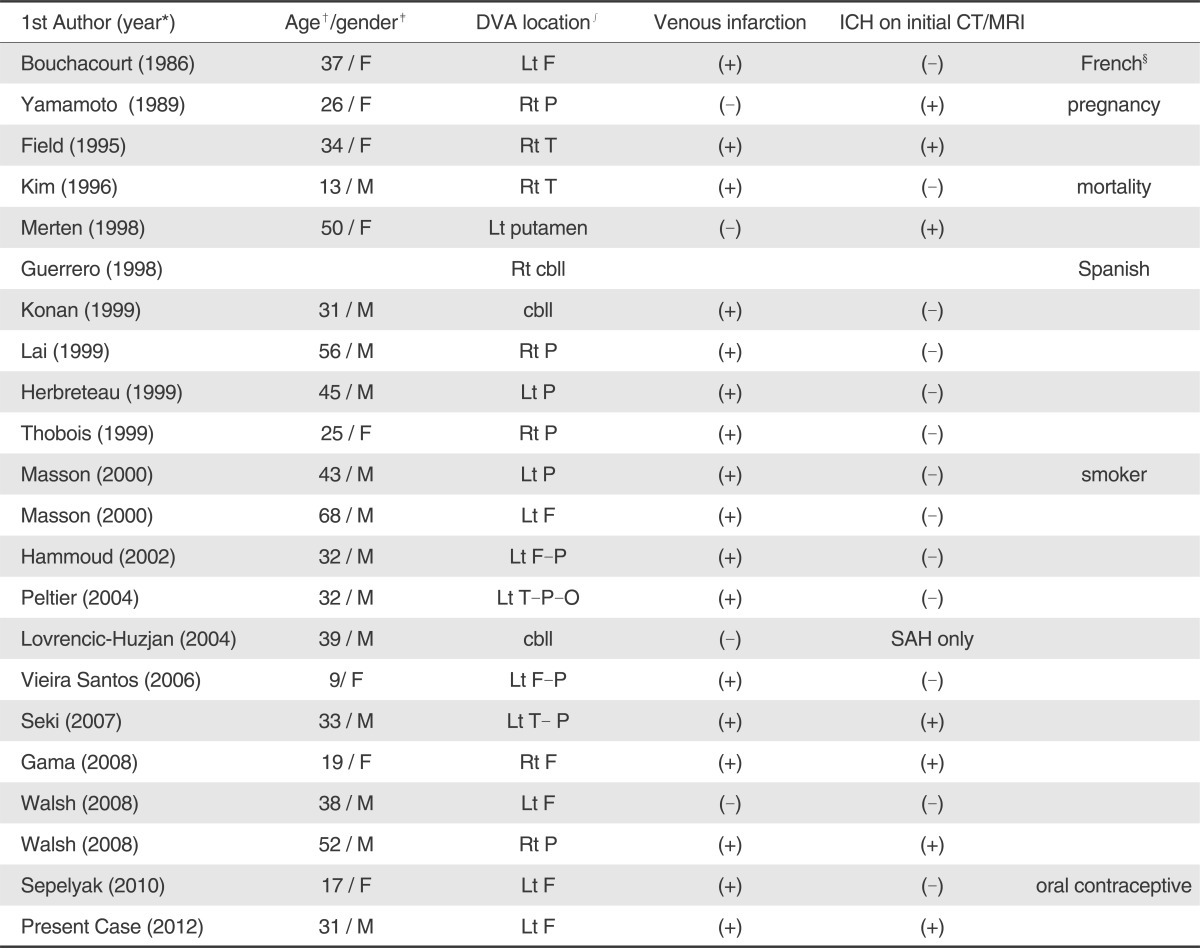
Among 21 cases of DVAs with venous thrombosis in the previous literatures, one was reported in French [13] and another one in Spanish [14]. 19 cases reported in English were reviewed [6, 9, 15-18] and we summarized their demographics, location of DVA, presence of parenchymal hemorrhage at the initial diagnosis including our case (Table 1). Among those 20, three had cerebellar DVAs [14, 18, 19], and one case presented with only with subarachnoid hemorrhage and no infarction [18]. Two cases had ICH only [8, 12] and f ive cases [7, 9, 15, 16] showed findings of ICH and venous infarction on the initial brain images. Most of them presented only CT, MRI or angiographic images at the initial diagnosis or at certain time points. Only four cases [7, 10, 12, 20] had follow-up images of any sort, but they did not show sequential changes of the thrombosed vein and DVA, neighboring brain tissue.
As described elsewhere, thrombotic obstruction of DVA and draining vein resulting venous congestion should be the pathologic mechanism for the initial parenchymal hemorrhages and venous infarction. In the present case, sequential CT, CT angiography and digital subtraction angiography demonstrated initial thrombotic obstruction of the venous drainage from DVA, its recanalization and temporal changes occurring in the affected brain parenchyma.
 XML Download
XML Download