

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Although intravenous (IV) recombinant tissue plasminogen activator (rt-PA) is still the f irst line treatment in acute ischemic stroke up to 4.5 hour time window, endovascular treatment might be superior to IV-rtPA alone to achieve revascularization in cases of large vessel occlusions. Among the several available devices for mechanical thrombectomy, mechanical thrombectomy using Solitaire stent (Covidien/ev3, Dublin, Ireland) has demonstrated high efficacy for successful recanalization of large artery occlusion in acute ischemic stroke [1, 2]. However, failure of mechanical thrombectomy to achieve successful revascularization has been reported in 20-30% of treated cases. In cases resistant to mechanical thrombectomy, several techniques have been introduced as a rescue method including the use of other stent retrievers, intraarterial thrombolysis, stent implantation [3], balloon angioplasty [4] and double Solitaire mechanical thrombectomy [5]. Here, we present our experiences of another rescue technique in which adjunctive tirofiban was injected through temporarily deployed Solitaire stent after failure of initial mechanical thrombectomy. We evaluated the feasibility, safety, and angiographic and clinical results of this technique.
MATERIALS AND METHODS
Patients
In this retrospective study, a consecutive series of patients was identified from stroke database of our hospital. From March 2013 to October 2014, we collected patients treated with adjunctive tirofiban injection during solitaire stent deployment after failure of initial trial of mechanical thrombectomy using Solitaire stent. During study period, a total of 96 mechanical thrombectomy procedures for large artery occlusions were performed at our hospital. Among them, 18 patients received adjunctive tirofiban injection during mechanical thrombectomy using Solitaire stent.
Prior to mechanical thrombectomy, CT and MRI were performed to evaluate the salvageable brain tissues and the presence of absence of intracranial hemorrhage. All patients underwent diffusion, perfusion imaging, and CT or MR angiography. When no other contraindications existed, a bridging IV-rtPA treatment was initiated after imaging study.
The indications for endovascular therapy were as following: 1) clinical diagnosis of acute stroke; 2) baseline National Institute of Health Stroke Scale (NIHSS) score >4; 3) intracranial large artery occlusion; 4) definite diffusion-perfusion or diffusion-clinical mismatch, 5) no intracranial hemorrhage.
Mechanical thrombectomy procedures
All procedures were performed under local anesthesia with/without sedative agents. A 6F Envoy guiding catheter (Codman, Raynham, MA) into a shuttle catheter (Cook Medical Inc., Bloomington, IN) or 9F Optimo balloon tipped guiding catheter (Tokai Medical Products, Aichi, Japan) was coaxially placed in the proximal extracranial vessel. The guiding catheter was continuously flushed with heparinized saline.
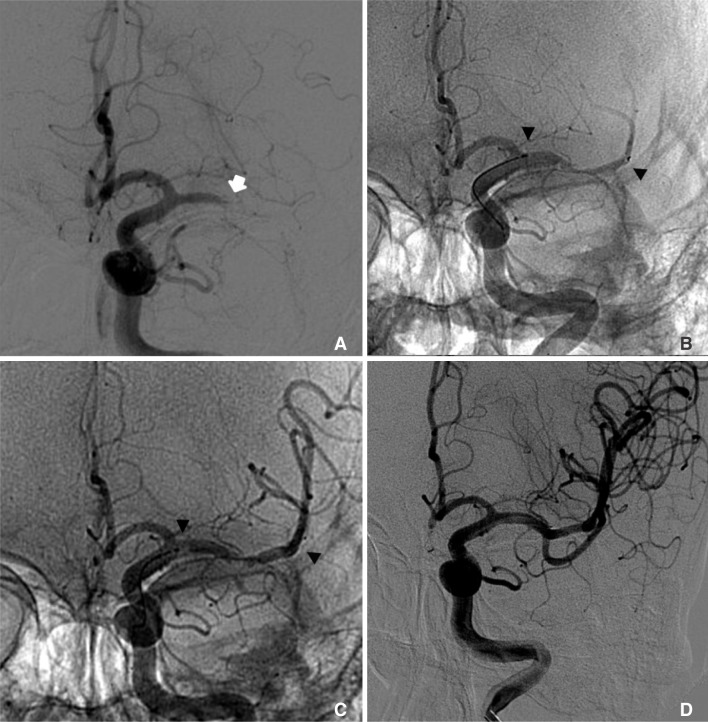
A Prowler select plus catheter (Codman & Shurtleff, Inc., Raynham, Massachusetts) with a Synchro 0.014 microguidewire (Stryker, Fremont, California) was navigated distal to the thrombus. Then Solitaire stent was deployed across the clot. The stent was kept deployed for 5 or 10 minutes before retrieving it. The partial re-sheathed Solitaire stent and the delivery microcatheter were gently withdrawn through the guiding catheter. While retrieving, proximal aspiration with a 50 cc syringe was performed through the guiding catheter. Immediate follow-up cerebral angiography was performed to assess recanalization. When one or more attempts of mechanical thrombectomy using Solitaire stent were failed, adjuvant injection of tirofiban through deployed Solitaire stent as a rescue method. Adjuvant tirofiban was injected 0.1 mg per a minute through microcatheter holding Solitaire stent. Then Solitaire stent and delivery microcatheter was withdrawn. Failure of initial thrombectomy was determined by individual operator's discretion. Example of the procedure is presented in figure 1. If successful recanalization did not occur, Solitaire thrombectomy was repeated according to operator's discretion.
Outcome measures and follow-up
The target vessel recanalization was assessed in the cerebral angiography and classified by using TICI score. Neurological improvement was assessed using NIHSS score at day 7. Neurological improvement was defined as improvement of NIHSS score more than 4 points. Functional outcome was assessed by mRS score at day 90. All patients underwent CT scan immediately after the procedure to evaluate hemorrhagic complications. Diffusion imaging and CT or MR angiography were performed within 24 hours and 7 days after thrombectomy. Complications associated with mechanical thrombectomy procedures including distal migration of emboli and post-procedural hemorrhage were investigated.
RESULTS
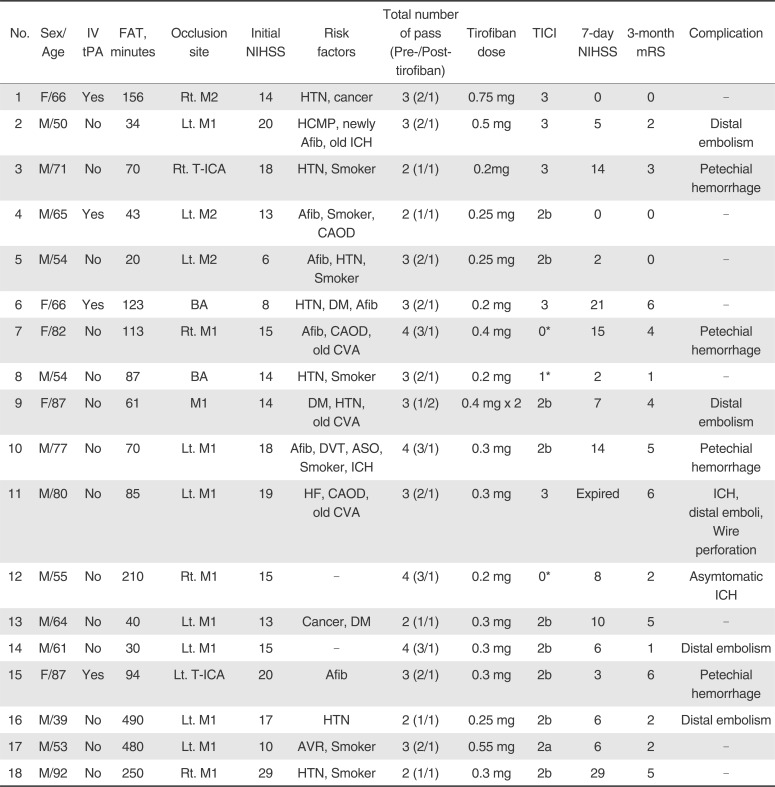
Baseline characteristics, procedures, and clinical outcomes are shown in Table 1. Median age and initial NIHSS score was 67 years (range, 50-92) and 15 (range, 6-29). Mean time of first found abnormal time was 233 minutes. Fourteen patients had occlusions in the middle cerebral artery, 2 in the distal internal carotid artery, and 2 in the basilar artery. Four patients were treated with IV rt-PA before the mechanical thrombectomy.
In 16 of 18 patients, Solitaire stent was used as first line device for mechanical thrombectomy. Manual aspiration thrombectomy with Penumbra reperfusion catheter was performed prior to Solitaire thrombectomy in 2 patients. Two patients received emergent carotid artery stenting prior to intracranial recanalization therapy for treatment of occlusion of cervical ICA. The mean dose of tirofiban used was 0.33 mg (range, 0.2-0.75 mg).
Successful recanalization was achieved in 14 (77.7%) of 18 patients after intraarterial injection of tirofiban and subsequent Solitaire thrombectomy. Three patients without successful recanalization received balloon angioplasty with a Gateway balloon catheter (Boston Scientific, Fremont, California) and stenting with a Wingspan stent (Boston Scientific, Fremont, California) and achieved successful recanalization. Thus, overall successful recanalization was achieved in 17 (94.4%) of 18 patients. Before injection of intra-arterial tirof iban, the mean number of passage of Solitaire stent was 1.9 (range, 1-3). After tirofiban injection, the number of passage of Solitaire stent to achieve successful recanalization was one.
Neurological improvement (decrease of NIHSS score more than 4 points) at 7 days was observed in 13 patients (72.2%). Good functional outcome (mRS ≤ 2) was observed in 9 patients (50.0%) at 3 months. Periprocedural complications occurred in 5 patients (5 distal migration of emboli and 1 vessel perforation). One patient with vessel perforation by microguidewire died of massive intracranial hemorrhage the day after the procedure. Overall, the mortality rate was 16.6% (3/18). Other fatalities were not directly related thrombectomy procedure. The one fatality was caused by malignant edema following large cerebellar infarction despite of successful recanalization of basilar artery. The other one was due to recurrent stroke.
DISCUSSION
In our case series, intra-arterial injection of tirofiban through a temporarily deployed Solitaire stent was promising because it is simple and has ability to achieve a high rate (77.7%) of recanalization in refractory cases. Good outcome rate (50%) in this study was comparable with those of randomized clinical trials of mechanical thrombectomy with Solitaire stent [1, 2].
The Solitaire stent is a self-expanding stent retriever designed to restore blood flow in patients with ischemic stroke due to large intracranial vessel occlusion and has yielded high rates of reperfusion and favorable clinical outcomes in patients with acute ischemic stroke [1, 6, 7, 8]. Despite higher recanalization rates of 61-85% [1, 2, 4, 8], not a few patients are still left without sufficient recanalization after mechanical thromectomy using Solitaire stent. Several different techniques to treat refractory cases to mechanical thrombectomy using stent retriever have been previously introduced. One case series showed that balloon angioplasty is an effective procedure when recanalization failed with Solitaire stent alone [4]. In study of Kurre el al. [3], other rescue methods were applied including the use of different stent retrievers, balloon angioplasty, permanent implantation of a stent, distal aspiration without a retriever and intra-arterial fibrinolysis. Klisch el al. [5] recently reported a 80% of successful recanalization and 50% of good clinical outcome in patients who had rescue treatment with double Solitaire stent retriever technique.
Tirofiban is a fast-acting, fast-deactivated, highly selective glycoprotein IIb/IIIa antagonists approved by Food and Drug Administration for the treatment of acute coronary syndrome up to 48 hours after onset.9 Tirofiban block the fibrin-binding receptors reversibly and effectively to prevent platelet aggregation. In the Safety of Tirofiban in acute Ischemic Stroke (SaTIS) trial, tirofiban is safe in acute moderate ischemic stroke even when administered within 3 to 22 hours after symptom onset and might save lives in the late outcome [10].
The benefits and risks of glycoprotein-IIb/IIIa inhibitor in patients receiving mechanical thrombectomy for acute stroke have been reported. Several case series showed that tirofiban was not associated with a significantly increased cerebral bleeding rate in patients with acute ischemic stroke [11, 12, 13]. However, in a recent observational study, patients who received tirofiban during mechanical thrombectomy for acute ischemic stroke had a higher risk of fatal intracerebral hemorrhage and poor outcome [14]. These findings should raise great caution in the use of tirofiban during mechanical thrombectomy for acute ischemic stroke. However, in latter study, tirofiban was infused via intravenous route continuously at least 12 hours after the intervention [14]. In our study, low-dose of tirofiban was infused briefly via intra-arterial route. Intra-arterial low dose tirofiban may achieve similar effect to intravenous administration of higher dose, which may decrease the risk of bleeding complications [11].
Even though a low dose tirofiban was used in our method, the application of this rescue method should only be made after careful consideration of various individual factors, such as the time from stroke onset, size of infarction core, blood pressure, known coagulopathy or prior use of antithrombotic medication. The limitations of the study are its small sample size, single center and retrospective nature.
 XML Download
XML Download