

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Frozen shoulder (FS) is characterized by the gradual onset and painful limitation of shoulder. First described by Duplay in 1872 as a condition that restricted abduction and external rotation, Codman subsequently expanded the definition of FS to include a gradual onset of shoulder pain, inability to sleep on the affected side, and limitation in both active and passive elevation and external rotation with a normal radiological finding [1].
The pathophysiology of FS includes chronic synovial inflammation followed by synovial tissue proliferation, thickening, and contraction [2]. Neviaser [2] reported that the most important pathology of the FS was a thickening and contraction of the joint capsule, which becomes adherent to the humeral head, thus causing limited joint mobility. However, some arthroscopic studies reported that no distinct intra-articular adhesion [23456]. Hannafin and Chiaia [7] described FS as four stages including preadhesive, freezing, frozen, and thawing incorporating both clinical and arthroscopic findings [7].
Treatment options for frozen shoulder range from conservative treatments including physical therapy, therapeutic exercise, joint mobilization and manipulation, nonsteroidal anti-inflammatory and opioid medications, intra-articular steroid and hyaluronic acid injections, suprascapular nerve block, glenohumeral distention arthrography with and without steroid supplementation, and manipulation under general anesthesia to surgical intervention [8]. Regardless of modality, the goal of conservative treatment for FS is to reduce pain, restore function and motion of the shoulder, and improve quality of life [8].
Distention arthrography (DA) is an effective treatment for freezing or frozen stage of FS, where intracapsular pressure and volume are gradually increased through injection of fluid with local anesthetics with or without steroid supplementation until capsular rupture [910]. Clinically effective joint mobilization and manipulation improves tissue extensibility, reduces soft tissue swelling and inflammation, reduces pain, increases range of motion (ROM), and stimulates peripheral mechanoreceptors in FS [11]. Interestingly, the combination of DA and manipulation under general anesthesia leads to a rapid decrease in pain and an improvement of shoulder range of motion in patients 4 to 6 weeks after intervention [12]. However, to the best of our knowledge, no study has compared the therapeutic effect of DA with translational mobilization (TM) with DA alone in FS. Therefore, the objective of this study was to evaluate the therapeutic effectiveness and safety of DA alone and in combination with modified TM for the treatment of FS.
MATERIALS AND METHODS
Patients and study design
This was a retrospective clinical study conducted with approval from the Institutional Review Board of Daegu Catholic University Medical Center (IRB No. CR-15-087). Informed consent was waived by the Institutional Review Board due to the retrospective nature of this investigation.
Eighty-five patients (51 females and 34 males; mean age, 63.3 years; range, 37–83 years) with unilateral idiopathic FS at freezing or frozen stages were recruited from the outpatient clinic of the Department of Rehabilitation Medicine.
Patients were eligible according to the following criteria: symptoms presented longer than 3 months, painful restriction of more than 30° in shoulder passive range of motion (PROM) in at least 2 of 4 movement directions (forward flexion, abduction, external rotation, and internal rotation) of the affected shoulder compared with the unaffected shoulder [13], capsular pattern of motion restriction (proportional limitation of the three passive glenohumeral motions including more limitation of external rotation, some limitation of abduction, and less limitation of internal rotation), and normal shoulder radiographic finding.
Patients were excluded according to the following criteria: full-thickness or large partial-thickness rotator cuff tendon tear on magnetic resonance imaging (MRI) or ultrasound, calcific tendinitis, significant glenohumeral arthritis on radiograph, previous shoulder injury and surgery, mastectomy due to breast cancer, hemiplegic shoulder pain due to stroke, systemic inflammatory disease such as rheumatoid arthritis, presence or suspicion of infection, uncontrolled diabetes mellitus (DM), severe osteoporosis of humeral head on radiograph, and bleeding tendency or use of anticoagulant medication.
All patients with FS (freezing or frozen stage) were diagnosed by medical history, physical examination, radiograph, and all patients were evaluated by ultrasound or MRI. The patients were consecutively allocated into two groups (the first term, 44 patients; the last term, 41 patients). Forty-one patients (21 females and 20 males; mean age, 62.2 years; range, 37–83 years) received DA with TM (group 1) and 44 patients (30 females and 14 males; mean age, 67.5 years; range, 44–76 years) received DA alone (group 2). DA and TM were performed only one time in all patients and TM was performed consecutively after DA. No significant difference in age was observed between the two patient groups. All patients received instruction for home-based exercise therapy for FS, but did not receive a physical therapy program. Lastly, use of nonsteroidal anti-inflammatory drugs (NSAIDs) was permitted following either procedure.
Distention arthrography
Before DA, a subacromial subdeltoid bursa was injected with lidocaine (1%, 6 mL) under ultrasound guidance [1415]. All DA procedures were performed by a single physiatrist (GY Park) with 25 years of experience in musculoskeletal rehabilitation. All patients were first placed in the supine position and put under local anesthesia with 2% lidocaine. A 21-gauge spinal needle was inserted at the anterior glenohumeral joint and advanced under fluoroscopic guidance. Correct placement of the spinal needle in the glenohumeral joint space was confirmed by injection of contrast medium (iopromide, Ultravist 300; Schering AG, Berlin, Germany). After confirming proper needle placement, a 16-mL solution (4 mL of 50 mg/5 mL of triamcinolone acetonide, 6 mL of 2% lidocaine, and 6–7 mL of 0.9% sodium chloride) was slowly injected. In patients with DM, 3 mL of 50 mg/5 mL of triamcinolone acetonide was used [16]. When resistance was felt during the injection, the injection was temporarily halted and subsequently resumed. DA was finished when the subscapular recess or long biceps tendon sheath were ruptured during the injection. If not ruptured after injection, shoulder PROM exercise was gently performed for 3 minutes by the physiatrist [17].
Translational mobilization
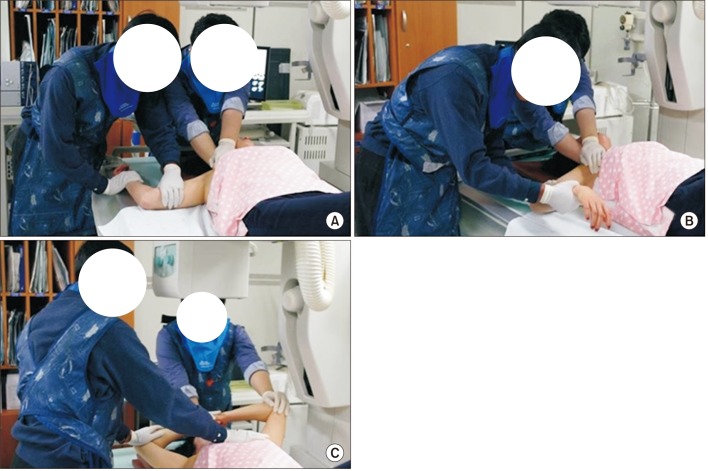
Modified TM with capsular stretching was performed once at 5 minutes after DA by the physiatrist in group 1 patients. The patients were placed in the supine position. First, the manipulator's one hand was placed on the humeral head as close to joint space as possible with the other hand grasping the proximal humerus. Inferior translation force was applied by one hand simultaneously with lateral traction of the humerus applied by the other hand, and shoulder abduction range was gradually increased to the end of available shoulder abduction. Second, shoulder external rotation range at 90° of abduction was gradually increased with lateral traction and posterior translation of the humeral head. Third, shoulder internal rotation range at 90° of abduction was gradually increased with lateral traction and posterior translation of the humeral head [18]. Last, Cyriax's capsular stretching was performed using mobilization technique. Briefly, the patient brought one hand to their forehead and placed the other hand on top of the first hand. The manipulator standing on the affected side put one of their hands on the sternum and the other hand on the distal arm of the affected side. The manipulator gently pushed the distal arm backwards to the end of the available range [19] (Fig. 1).
Clinical parameters
Clinical parameters including visual analog scale (VAS), Cyriax stage (score range, 1–4), and shoulder PROM (forward flexion, abduction, external rotation, and internal rotation) were measured at baseline, 1 month, and 3 months after the treatment by the other physiatrist. The degree of shoulder pain was assessed using the 10-cm pain VAS, where 0 indicates ‘no pain’ and 10 ‘worst pain possible’ [20]. The passive forward flexion and abduction of shoulder were measured with the patient in the supine position, and passive external and internal rotations were measured at 90° of abduction with scapular stabilization in supine position. Cyriax stage was assessed on a grade from 1 to 4 according to four criteria: the first three were provided by the clinical history of the patient (pain at rest, patient can lie on the affected side at night, and pain spread below the elbow) and the fourth was the end-feel during external rotation of the shoulder [19]. All outcome parameters were measured before treatment and at 1 and 3 months following intervention.
Complication assessment
Follow-up ultrasound of the affected shoulder was performed by the physiatrist with 25 years of experience in musculoskeletal ultrasound immediately after DA with TM to identify potential complications associated with intervention.
Statistical analyses
Statistical analyses were performed using SPSS version 19.0 (IBM Corporation, Armonk, NY, USA), with the level of significance set at p<0.05. Independent t-test was used for the difference of age, symptom duration, and four shoulder PROMs between two groups. The Mann-Whitney U-test was used for VAS and Cyriax stage, and the chi-square test was used for gender, affected side, the presence of DM at baseline. Repeated measures analysis of variance (ANOVA) was used to examine the intragroup differences for effect of time. Intergroup differences in the outcome measurements were evaluated using Mann-Whitney U-test. The post-hoc power analysis was performed using G*Power 3 (Heinrich-Heine-University, Dusseldorf, Germany) and the power (1−β) was 0.47–0.99.
RESULTS
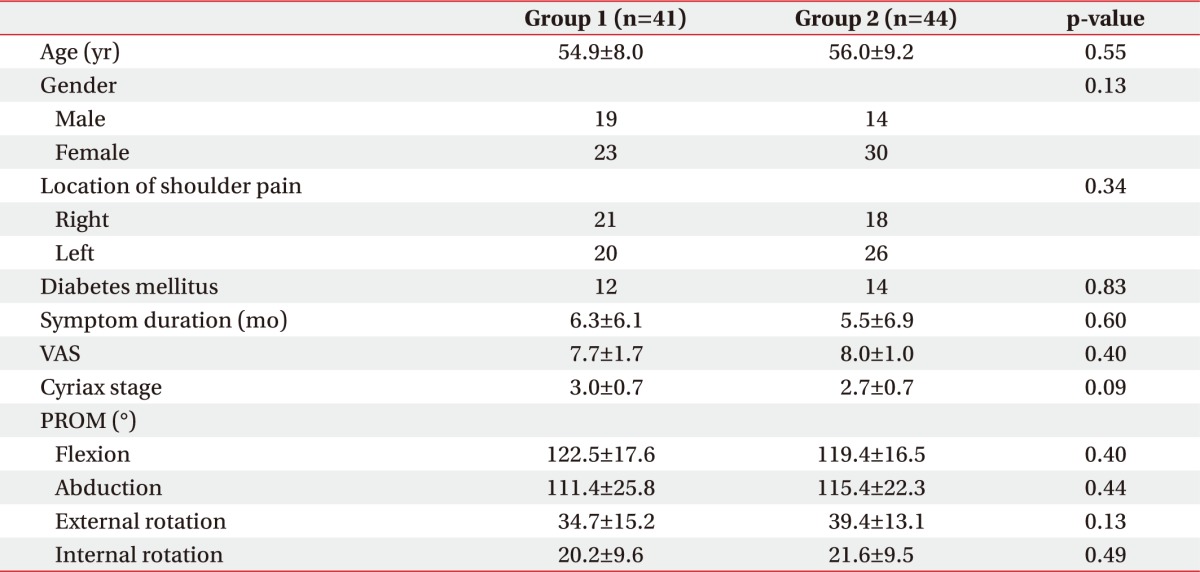
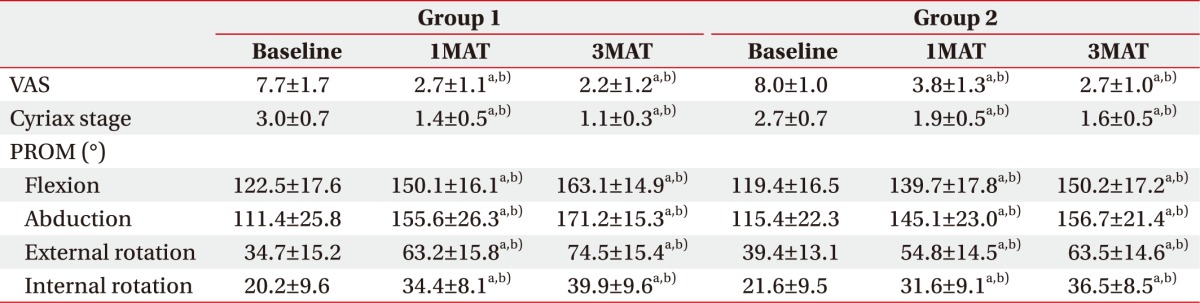
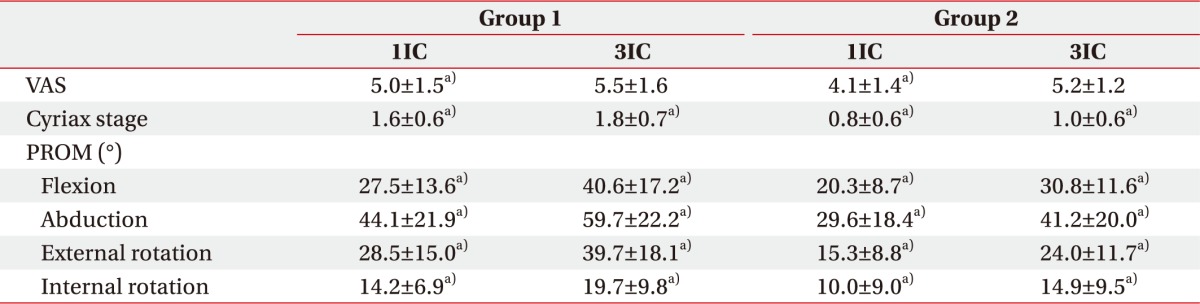
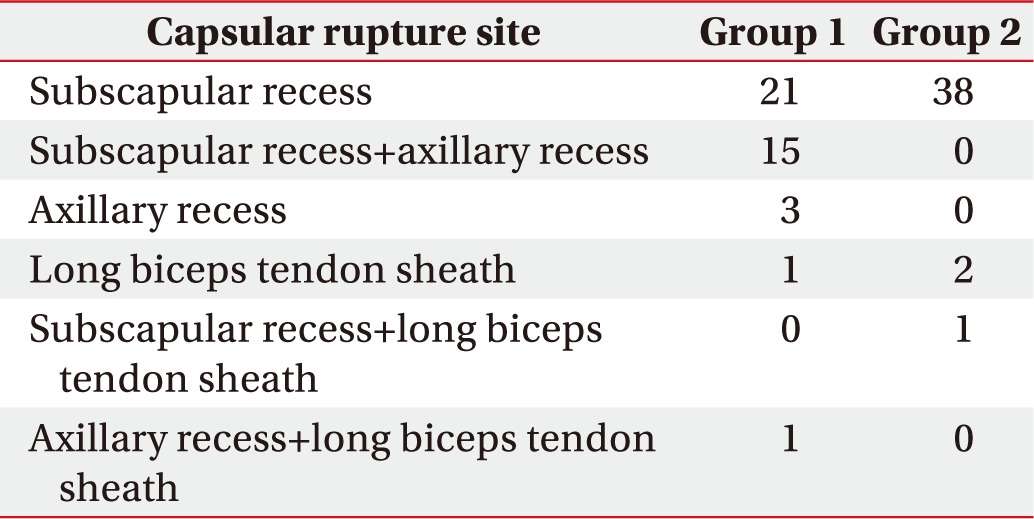
At baseline, there were no significant differences in patient gender, affected side, symptom duration, presence of DM, and all clinical parameters including VAS score, Cyriax stage, and shoulder PROM between the treatment groups (Table 1). All clinical parameters were significantly improved in both groups at all post-treatment time points compared to baseline parameters (p=0.000) (Table 2). However, all mean PROMs at 1 and 3 months following treatment were significantly greater in FS patients receiving DA and TM therapy—flexion at 1 and 3 months after treatment (1/3MAT) (p=0.008 and p=0.047), abduction at 1/3MAT (p=0.038 and p=0.000, external rotation at 1/3MAT (p=0.009 and p=0.009), internal rotation at 1/3MAT (p=0.045 and p=0.049) (Table 2). Relative to DA alone, the combination of DA and TM therapy also significantly decreased mean VAS score and Cyriax stage in FS patients at one and three months post-intervention—VAS at 1/3MAT (p=0.000 and p=0.032), Cyriax stage at 1/3MAT (p=0.002 and p=0.000) (Table 2). The mean interval change of clinical parameters between baseline and at 1 and 3 months (1/3IC) after treatment were significantly greater in patients receiving the combination DA and TM therapy—VAS 1/3IC (p=0.031 and p=0.243), Cyriax stage 1/3IC (p=0.000 and p=0.000), flexion 1/3IC (p=0.008 and p=0.031), abduction 1/3IC (p=0.001 and p=0.000), external rotation 1/3IC (p=0.000 and p=0.000), internal rotation 1/3IC (p=0.007 and p=0.000) (Table 3). Capsular rupture sites in patients receiving both DA and TM were as follows: 21 subscapular recess ruptures, 15 subscapular and axillary recesses ruptures, 3 axillary recess ruptures, 1 long biceps tendon sheath rupture, and 1 axillary recess and long biceps tendon sheath rupture. Conversely, patients receiving DA alone presented 38 subscapularis recess ruptures, 2 long biceps tendon sheath ruptures, and 1 subscapularis and axillary recesses rupture (Table 4). No serious complications, such as fracture, glenohumeral dislocation, peripheral nerve injury, rotator cuff tear, and infection, were observed following either treatment.
DISCUSSION
The results demonstrate that the combination of DA with TM is a safe and effective treatment to reduce persistent pain and restricted mobility found in patients with freezing or frozen stage FS. Additionally, all clinical outcome parameters including pain (VAS score), PROM, and Cyriax stage were significantly improved at one and three months following DA alone, consistent with previous studies [2122]. In unafflicted patients, normal shoulder joint capacity was greater than 16 mL, whereas it was less than 10 mL in patients with FS [23]. Mao et al. [24] reported the correlation between shoulder joint space capacity and shoulder ROM. Both the shoulder ROM including flexion, abduction, external rotation, and internal rotation and the shoulder joint capacity measured by arthrography were significantly increased after conservative treatments including physical modalities and exercise. However, the increased shoulder joint capacity was only significantly correlated with increased external rotation. DA combined with steroid injection revealed better improvement of shoulder ROM than steroid injection alone in patients with FS [21]. Furthermore, steroid injection with repeated DA was more effective in reducing patient disability and pain compared with a single DA treatment [22].
Placzek et al. [25] reported the long-term effects of translational manipulation about ROM, function, and pain in patients with FS and concluded that translational manipulation is a valid, biomechanically excellent treatment for FS. The same authors also reported increased shoulder ROM and decreased pain at 14 months after translational manipulation in FS, and typical cracking sound known as characteristic crepitus could be heard during manipulation. This sound was believed to reflect the loosening and tearing of the adhesive shoulder joint capsule [2627]. Although not directly associated with pain relief, this cracking sound was correlated with improvement of shoulder external rotation [28]. In our study, the manipulator experienced the cracking sound during TM with shoulder external rotation in most cases and the increased ROM immediately after cracking sound [29].
Combination treatment using DA with manipulation under general anesthesia was first reported by Ekelund and Rydell [12] and resulted in a rapid decrease in pain and increase in shoulder ROM at 4 to 6 weeks after intervention. The combination of DA and manipulation under local anesthesia provided sufficient improvement in shoulder ROM, and was regarded as a safe and effective treatment for FS [30]. Choi et al. [28] reported that DA with manipulation in FS patients led to a reduction in pain and improvements in both shoulder ROM and general function. In agreement with the previous studies, our data indicate that DA with TM resulted in significant improvements in all clinical parameters including VAS, Cyriax stage, and all shoulder PROMs at 1 and 3 months following treatment.
Additionally, the interval change of all clinical parameters was significantly greater in FS patients receiving DA with TM than those receiving DA alone. As a possible explanation of this finding, TM combined with DA might effectively resolve the residual deficit in shoulder motion present following DA alone. In our study, subscapular recess was usually ruptured after DA alone, but axillary recess was ruptured together with subscapular recess rupture after DA with TM.
Instead of manipulation requiring general or local anesthesia via suprascapular and/or axillary nerve block, we performed a modified TM technique with capsular stretching after DA. For pain control during DA and DA with TM, subacromial subdeltoid bursa was injected with local anesthetics before the treatments. Uncontrolled shoulder joint manipulation may cause structural damage to cartilage and soft tissue of the glenohumeral joint. Furthermore, manipulation under general anesthesia in FS can cause iatrogenic injury, such as humeral neck fracture, axillary or radial nerve injury, superior labrum anterior-posterior lesion, partial-thickness tear of rotator cuff tendon, labral detachment, and glenohumeral ligament tear [12]. In our study, no serious complications were associated with either procedure as assessed by ultrasound following treatment. There are several possible explanations for this finding. First, DA will reduce capsular adhesion of FS before TM, protecting the soft tissues surrounding the shoulder during TM. Second, instead of manipulation, we employed a short lever mobilization technique. Contrary to traditional long lever angular manipulation, short lever mobilization of the shoulder will reduce the inflicting force applied to the shoulder during treatment. Finally, all procedures were performed by the skilled physiatrist with 20 years of experience in manual medicine.
There are several limitations to this study. First, the sample size was relatively small. Therefore, serious complication could not happen because of the small number of patients. Second, the follow-up period after treatment was short. Third, this was a retrospective study and we cannot exclude the possibility of inherent patient selection bias. However, this is the first study to compare the therapeutic effect of DA alone with combination DA and TM therapy in FS patients. Further prospective study with a larger sample size, long-term follow-up, and double-blinded control will be necessary to confirm the validity of our study results.
In conclusion, the combination of TM with DA significantly decreased shoulder pain and increased shoulder PROM without serious complications in patients with freezing or frozen stage FS. Furthermore, compared to DA alone, our results indicate that DA in combination with TM may be more therapeutically effective for FS treatment.
 XML Download
XML Download