

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neck pain is becoming increasingly common throughout the world [1], and the annual incidence of cervical herniated nucleus pulposus (HNP) being 83.2 out of 100,000 persons [2]. Since the cervical spine is involved in a wider range of motion and is a functionally more active structure than the lumbosacral spine, pain and limitation in the range of motion leads to substantial discomfort and complications [3]. Despite the fact that most HNPs of cervical spine are smaller in size and in a protruded form compared to lumbar HNPs, the chance of developing neurologic or radicular symptoms are higher in cervical spine, since the spinal canal and neural foramen are also smaller [4]. Thus, lesions involving cervical spine can lead to secondary impairment, causing major limitations in daily life.
Although many symptoms are alleviated by medical and physical therapies, structurally unstable lesions involving the spinal nerve root or cord can cause severe pain, and often require surgical intervention. However, the role of surgical approaches for the treatment of cervical HNP remains the subject of much debate. Due to the complex structure of blood supplies and nerves in the cervical regions, surgeries often lead to serious complications, similar to other high risk procedures involving artificial graft and implant insertions [56]. Since there is no definite evidence supporting the superiority of surgical intervention over non-surgical treatments, the correct approach to cervical HNP remains controversial [7].
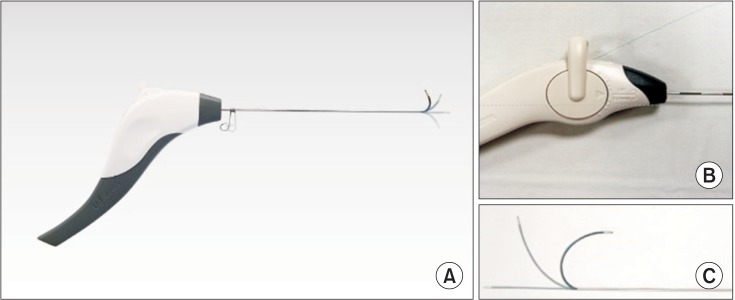
There are numerous non-surgical interventional approaches to treat cervical HNP. Most methods involve approaching the spinal disc directly and cauterizing parts of the spinal disc using various modalities [89]. Even though non-surgical interventions minimize secondary damage to other tissues and avoid general anesthesia, most methods require further extensive studies to explain their mechanism of action and demonstrate their effectiveness. A common and minimally invasive percutaneous decompression device, Nucleoplasty (ArthroCare Co., Sunnyvale, CA, USA) [10], uses radiofrequency ablation to remove a minimal amount of nuclear tissue with the hope that a small decrease in volume will result in a large decrease in pressure. Although the efficacy and safety of disc ablation with radiofrequency energy has been previously demonstrated, focal direct removal of the herniated disc is restricted by the inability to navigate the catheter within the herniation. To overcome this liability, we developed a navigable decompression device named L'DISQ-C (U&I Co., Uijeongbu, Korea) that is designed to allow direct access to the herniated disc material by rotating a control wheel (Fig. 1). A previously published study of L'DISQ, on patients with lumbar disc herniation, showed results of considerable improvement in pain and decrease in disabilities [12]. The current study aimed to assess the clinical efficacy and safety of selective focal ablation using navigable disc decompression device for patients with cervical HNP.
MATERIALS AND METHODS
This study was approved by Korea University Medical Center ethics committee (MD13023-002). It progressed prospectively with patients who were thoroughly explained the procedure and signed the informed consent. All procedures were performed by the physician who had invented the device and designed the procedure, and clinical assessment and data analysis were carried out by other physicians.
Subjects
A total of 795 patients with posterior cervicalgia and upper extremity pain due to cervical HNP, were enrolled from June 2009 to September 2013. We recommended the procedure to patients with little or no improvement of pain after at least one month of conservative management, including physical therapy, oral analgesics, and cervical epidural steroid injection with dexamethasone (4 mg/mL) and 0.5% lidocaine under fluoroscopic guidance.
Following were the exclusion criteria for the study: clinically significant cervical HNP of two or more levels on magnetic resonance imaging (MRI); severe degeneration of the target disc on MRI; cervical myelopathy on MRI and any signs of upper motor neuron lesion upon physical examination, symptom-related cervical bony malformation, prior cervical spinal surgery history; conjoined shoulder joint problem, symptom-related psychologic disorder, hematologic disorder, and musculoskeletal painful conditions (fibromyalgia, myopathy, polyneuropathy). Of the initial 795 patients, 775 patients were excluded on basis of the reasons noted above. The remaining 20 patients underwent percutaneous cervical disc decompression with L'DISQ-C after having signed the informed consent. All patients were allowed to be treated conservatively with analgesics and physical therapy during the 48 weeks after the procedure, excepting for steroid injections. Most of them received physical therapy, including heat therapy.
Device and patient preparation
A report published in 2011 describes the therapeutic efficacy of a newly developed navigable percutaneous disc decompression device in patients with lumbar HNP and radicular pain [12]. The device approaches the herniated disc tissue through the intradiscal course with considerable accuracy, and ablates a part of the tissue for decompression by high energy plasma particles.
We modified this device to an applicable form named L'DISQ-C for entering into the cervical intervertebral space (Fig. 1). This device has a wand of shorter length and smaller diameter than of the lumbar catheter, which facilitates insertion into the narrow cervical intervertebral disc space and lends stability to anchor round the neck contour. Navigable range, generating ability of plasma and other component materials are similar to the lumbar catheter.
We injected 1.0 g of cefazolin intravenously, 30 minutes prior to the procedure to decrease the incidence of infection. Blood pressure, heart rate, electrocardiogram, oxygen saturation, and respiration rate were monitored during the procedure. Patients were placed in the supine position with the neck extended gently by placing a cushion beneath the shoulder. A soft strap was placed over the forehead for stabilization. Patients were asked to gently distract both shoulders downward to the operation table. The neck was prepped and draped in a sterile fashion. An aseptic technique was used throughout the procedure. Deep sedation was prevented so that complete neurological monitoring of the patient was possible during the entire procedure.
Procedure techniques
All procedures were performed by a single physician, an expert in spine procedures, with two assistants. The procedure was performed under fluoroscopic guidance using a standard oblique intradiscal approach used for cervical discography [13]. During the initial stage, fluoroscopic examination identified the target disc and an appropriate skin site for needle trajectory. The introducer needle was advanced, taking care to avoid the puncture of tracheoesophagus and major vessels including the carotid artery. The trachea was displaced medially and vessels laterally using two digits applied with firm pressure to the space between the trachea and the medial border of the sternocleidomastoid muscle. Pulsations of the carotid artery were felt by the fingers at the lateral side, thus avoiding puncturing the major vessel and prevent bleeding. After encountering the anterior cervical spine, an introducer needle passed contralateral to the herniation, and a 25-gauge spinal needle tip was placed on the posterior wall of the ipsilateral foramen at its middle third. Another needle was used for epidural saline infusion to protect the dura and nerves from heat damage. After confirming the needle tip placement at the center of the disc with anteroposterior (AP) and lateral fluoroscopic views, the stylet of the introducer needle was withdrawn from the cannula and replaced with a flexible 1.0 mm diameter wand. By manipulating the control wheel, we advanced the wand tip to the herniated portion. After connecting the cervical wand to the power generator, we tested the electrical conductivity to the nerve fibers before each ablation, for any complaint of electrical shock-like pain or muscular contraction; if required, the tip was withdrawn and retested. From this brief test of electrical stimulation, we were able to prevent severe neural tissue damage. We used brief bursts of 50–75 W for 2 seconds to ablate disc tissue. After each ablation, the wand was slightly repositioned and after the test stimulation, ablation was repeated for a total of 100–150 seconds.
Assessment of final tip placement
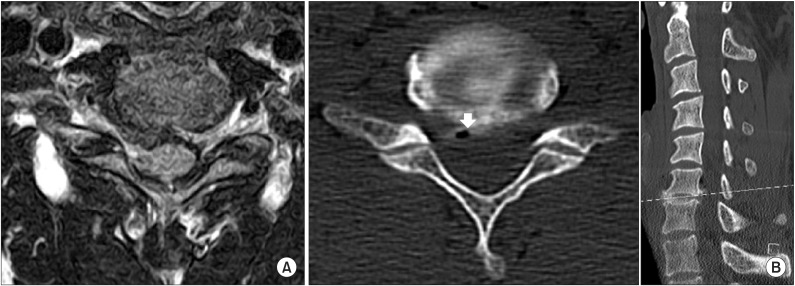
The target point was established through MRI analysis before the procedure. On the sagittal and axial planes of the significant HNP, the space between the herniated base and outline was decided as the target area for ablation (Fig. 2A). Using C-arm fluoroscopy by AP and lateral views during the procedure, the intradiscal location of the wand tip was confirmed and saved as image files (Fig. 2B, C). We measured the location of the wand tip through image analysis just after the procedure, without knowing the symptomatic effect or clinical outcomes of the subjects.
After the procedure, the MRI and C-arm images were structurally matched through the bony markers—anterior and posterior vertebral lines, spinolaminar line, adjacent endplate lines, spinous process line, and lateral vertebral lines (Fig. 2). We defined the wand position as being in ‘correct’ position if the tip was placed within the target area of both AP and lateral views, and as ‘incorrect’ if otherwise.
Clinical outcome measures
Assessments performed included a Numeric Rating Scale (NRS), Neck Disability Index (NDI) and Bodily Pain scale of Short Form-36 version 2 (SF-36 BP). NRS rates the severity of pain as a score between 0 and 10. NDI is the method of assessment for disability affected by neck pain. The higher the NDI scores, the more severe the disability. SF-36 BP is one section of the Short Form-36 Health Survey version 2, which measures the health status and is a patient-reported survey. The ‘bodily pain’ section describes the limitation in daily life due to pain, and lower the score, more severe is the disability. Data were obtained before the procedure and at follow-up visits scheduled at 1, 4, 12, 24, 48 weeks after the procedure, through face-to-face or telephone consultations. A successful outcome was defined as reduction of NRS by more than 50%.
To identify the ablated portion of the disc and other visible complications, post-procedural computed tomography (CT) studies were taken. The CT images were obtained just after the procedure and was assessed by a specialized radiologist.
Statistical analysis
The Friedman test was carried out to compare the clinical outcomes before and at each follow-up. The post hoc test was the Wilcoxon signed-rank test with Bonferroni correction. The correlation between the outcomes and tip placement was analyzed through the Fisher exact test at the 0.05 significance level. SPSS ver. 20.0 KO for Windows (IBM SPSS, Armonk, NY, USA) was used to evaluate the data.
RESULTS
Patient characteristics
The 20 consecutive patients who satisfied the enrollment criteria underwent focal cervical disc decompression that utilized a navigable wand. There were 12 males and 8 females, with a mean age of 45.4 years ranging from 28 to 65 years. The mean duration of symptoms was 5.6 months with a range of 1–20 months. The levels of the targeted disc were C3/4 in 1 patient, C4/5 in 2 patients, C5/6 in 6 patients, and C6/7 in 11 patients (Table 1). According to the MRI readings, disc protrusion was demon-strated in 10 patients and extrusion in 10 patients.
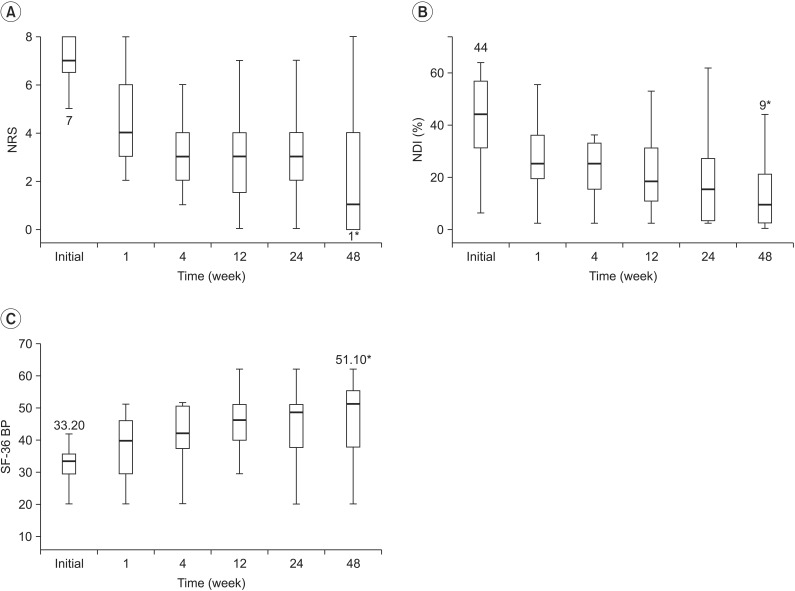
Clinical outcomes
Following the procedure, serial follow-up clinical data were obtained for all 20 patients for 48 weeks. Compared to the preoperative baseline, the NRS, NDI, and SF-36 BP scores showed statistical improvement at the postoperative 48 weeks follow-up (Fig. 3). The average reported pain level as measured by NRS was 7 before the procedure and 1 after 48 weeks. There was significant NRS improvement for the first 4 weeks (p=0.01) after the procedure. No further meaningful improvement was reported from 4 weeks to 48 weeks, but the initial improvement was sustained. NDI decreased significantly for one week postoperatively (p=0.01), and continued improving until 48 weeks, from 44 to 9 points. The SF-36 BP scale increased significantly for one week postoperatively compared to the baseline of 33.20 (p=0.02), and improved steadily to 51 at 48 weeks. Successful outcomes were reported in 16 patients (80.0%), with a reduction by more than 50% in NRS. Four subjects did not show any successful outcomes. One subject showed NRS decrement until post-24 weeks, but the symptom recurred between 24 and 48 weeks. The other 3 patients recorded incorrect tip placement. No intra-procedure or post-procedure complications were reported such as swallowing discomfort, hoarseness, esophageal perforation, vascular or nerve injuries, infection and cerebrospinal fluid leakage, during the follow-up period. On post-procedural CT images, some radiolucent spots were often identified in epidural and targeted intervertebral space, which were presumed to be vaporized air bubbles (Fig. 4). The bony structures and alignments were scanned and compared with pre-procedural MRI or simple X-ray images, but no specific changes were observed in any of the patients.
Final placement of the wand tip
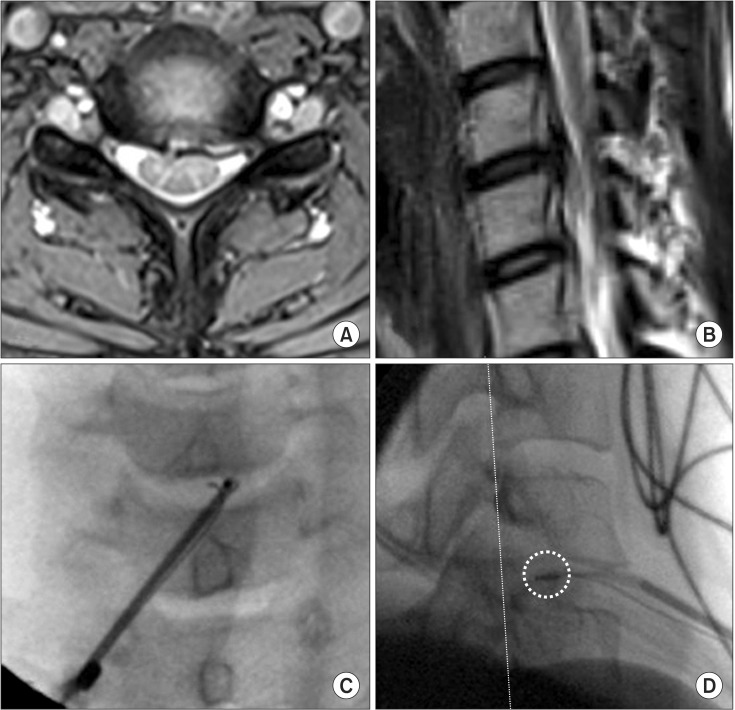
We confirmed the final placement of the wand tip by fluoroscopic AP and lateral views in all participants. The wand was passed beyond the disc margin and into the disc herniation. The location of the wand tip resulted in 16 correct and 4 incorrect placements. The wand tips of all incorrect cases were placed on more inner side beneath the herniated base (Fig. 5). Therefore, the tip could not approach the target area from the center of the disc. Unsuccessful outcomes were recorded for 3 incorrect and 1 correct tip case at post-48 weeks. Remaining correct tip placements significantly correlated with successful outcomes after 48 weeks (Table 2).
DISCUSSION
Open surgery for cervical HNP usually requires entering the spinal canal with the risk of complications such as epidural hematoma, dural tear, or surgical site infection with surgical hardware and dysphagia [51415]. In contrast to open surgery, minimally invasive cervical procedures reduce these complications and become an alternative treatment for cervical HNP. In the last decade, a variety of minimally invasive procedures, including mechanical, chemical, and thermal/heat (radiofrequency and laser) methods, have been developed to decompress the discs in patients with cervical HNP [1617]. Knight et al. [18] reported that cervical laser disc decompression produced and sustained significant clinical improvement in approximately 76% of cervical HNP patients throughout the period of 43 months. Richaud et al. [19] treated 38 patients with cervical HNP with percutaneous chemonucleolysis, and 83% of the group resulted in successful outcomes. Birnbaum [16] published a study regarding the clinical efficacy and safety of percutaneous decompression of cervical HNP using radiofrequency energy. These minimally invasive procedures have many benefits compared to open surgery—less damage to soft tissue and bone, no requirement of long convalescence, the ability to perform under local anesthesia on an outpatient basis, and the ability of the patient to return rapidly to daily life. All these interventional techniques try to relieve the nerve root or dural compression by ablating the herniated disc tissue.
We used radiofrequency-driven metal electrodes for focal cervical disc decompression using navigable wand to discharge plasma in saline solution. The localized plasma positioned near biological tissue can cause numerous reactions, such as tissue debulking or cutting. The hydroxyl radical generated through plasma plays the primary role in nucleus pulposus decomposition. Chen et al. [10] studied the effect of disc ablation on contiguous structures, and concluded that volumetric removal of target disc tissue could be achieved without damage to the adjacent nucleus, annulus, endplate, spinal cord, or nerve root.
However, the most recently developed percutaneous decompression devices that use plasma energy are designed to decompress the center of the nucleus rather than the herniated disc directly. Therefore, a comparatively large amount of tissue reduction in the central disc is required, and excessive disc tissue removal accelerates the disc degeneration and reduces the disc height [20]. To overcome this liability, our catheter is designed to directly ablate the focal herniated tissue. Designed to allow direct access to the herniated disc material, the device vaporizes the herniated nucleus using bipolar radiofrequency plasma. In contrast to the more percutaneous decompression devices that use a rigid and uncontrollable tip, the wand tip of our device is curved by rotating a control wheel and directed into the disc herniation. Direct and focal removal of the target herniated disc by the flexible and navigable tip may induce better clinical outcomes and avoid excessive disc degeneration. In our study, at sequential postoperative follow-ups, there were clinically significant reduction in pain, improvement of disability and health-related quality of life, consistent with previous studies due to the percutaneous cervical disc decompression by radiofrequency energy [2122].
Successful outcomes were observed in 80% of our patients, and this may be associated with the needle tip placement according to the analysis of the final placement of the wand tip. Among the 4 incorrect tip cases, 3 had unsuccessful outcomes throughout the period. As mentioned above, the needle tip was placed more on the inner side beneath the herniated base in ‘incorrect’ cases, and the tip could not approach the target area. An exact approach to the target area is essential for a successful outcome, and this was achieved by proper control of the navigable wand tip. Furthermore, targeted and focal ablation minimizes the amount of ablated disc tissue for decompression and injury to the outer annulus fibrosus. The proper amount of nucleus pulposus was also preserved, and decrease in the disc height was prevented. Therefore, it could maintain the loading resistance of the cervical disc and diminish the acceleration of disc degeneration. Eventually, the intrinsic distance between the two electrodes is 0.8 mm, a nerve root greater than 0.8 mm from the tip is theoretically safe from electric injury and the applied electric currents should pass to the other electrode rather than passing to the nerve root. In addition, the thin outer annulus membrane is a good conducting barrier of electrical current, which theoretically reduces neural damage due to the bipolar electrical current [12]. Furthermore, the highest temperature recorded during controlled ablation is 40℃ to 60℃, with a rapid decline in temperature with distance [23]. Therefore, adjacent and surrounding healthy tissues are safe from thermal elevation. It is, however, crucial that the practitioner should be careful when manipulating the device to prevent severe neural tissue damage. Before each ablation, a brief electrical stimulation test is recommended. If stimulation or limb movement is detected, the wand must be repositioned. Forward movement of the wand during ablation must be prevented.
The limitation of this study was that it was a pilot study with a short-term follow-up and included few subjects. A randomized and controlled-study is required in the future. Comparisons of the clinical efficacy, depending on cervical levels or types of herniation, would be needed to ascertain the application of the percutaneous disc decompression with the navigable wand on various patients with cervical HNP. Despite these limitations, the promising results and safety of the procedure in this study encourages us to utilize this technique in well-selected cases.


 XML Download
XML Download