

 PDF
PDF ePub
ePub Citation
Citation Print
Print



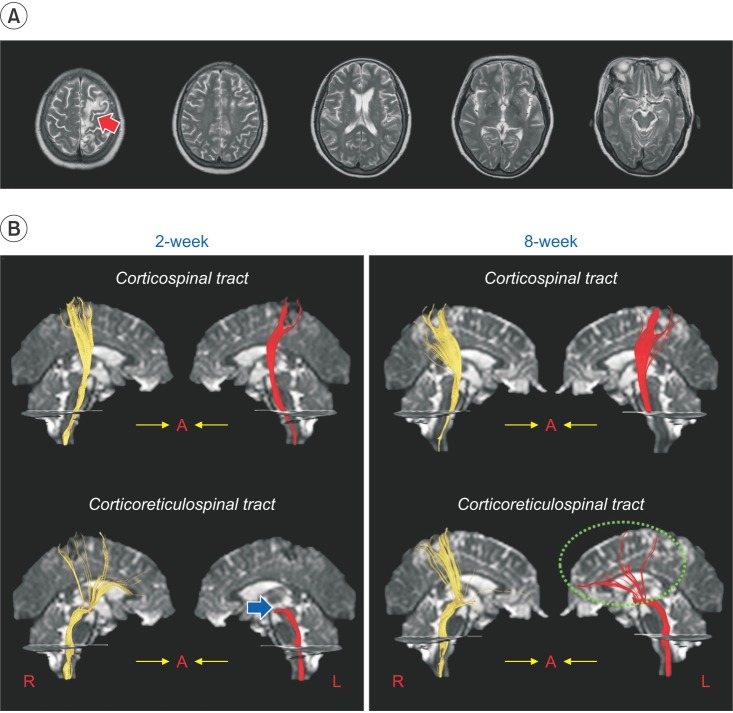
A 66-year-old right-handed female patient developed absolute weakness of the right lower extremity (Manual Muscle Test [MMT], 0/5), following an infarct in the left supplementary motor area and premotor cortex (Fig. 1A). She underwent conservative management at the neurology department of a university hospital. Two weeks after the infarct, she was transferred to the rehabilitation department of the same university hospital. The weakness of the right lower extremity was similar to that seen at the time of the infarct (MMT, 0/5). She underwent comprehensive rehabilitative management, including neurotropic drugs (pramipexole, amantadine, and venlafaxine), movement therapy, and neuromuscular electrical stimulation of the right knee extensor and ankle dorsiflexor muscles. After rehabilitation for 6 weeks, there was significant motor recovery of her right lower extremity (MMT: hip flexor, 3; knee extensor, 3; and ankle dorsiflexor, 0). At 8 weeks after the onset, she was able to walk independently on an even floor, fitted with an ankle-foot-orthosis.
Diffusion tensor imaging (DTI) data were acquired twice (at 2 and 8 weeks after the onset). DTI was performed using a sensitivity-encoding head coil on a 1.5-T. For analysis of the corticospinal tract (CST), the first and second regions of interest (ROIs) were placed at the anterior blue portion of the upper and lower pons, respectively, on the axial image of a color map. For reconstruction of the corticoreticulospinal tract (CRT), the first ROI was placed on the reticular formation of the medulla, and the second ROI was placed on the tegmentum of the midbrain. At the 2-week diffusion tensor tractography (DTT), the integrity of both the CSTs and the right CRT of the patient were preserved. However, the left CRT showed discontinuation at the brainstem level (Fig. 1B). By contrast, the 8-week DTT revealed the discontinued left CRT was connected to the left cerebral cortex (the changes of the DTT parameters are described in Supplementary Table S1).
The 2-week DTT showed that the left CRT was discontinued at the brainstem level, suggesting severe injury of the left CRT, which may have degenerated following injury due to the left cerebral infarct. Elongation of the discontinued left CRT to the cerebral cortex on 8-week DTT appears to indicate a recovery of the injured left CRT. We believe this recovery of the left CRT is partly attributed to the motor recovery of the right lower extremity in this patient. In conclusion, using DTT, we hereby demonstrate the recovery of an injured CRT in the affected hemisphere of a patient with a cerebral infarct, concurrent with the motor recovery of the affected lower extremity [1234].
 XML Download
XML Download